The role of the trabecular meshwork in eye fluid drainage

What is the trabecular meshwork?
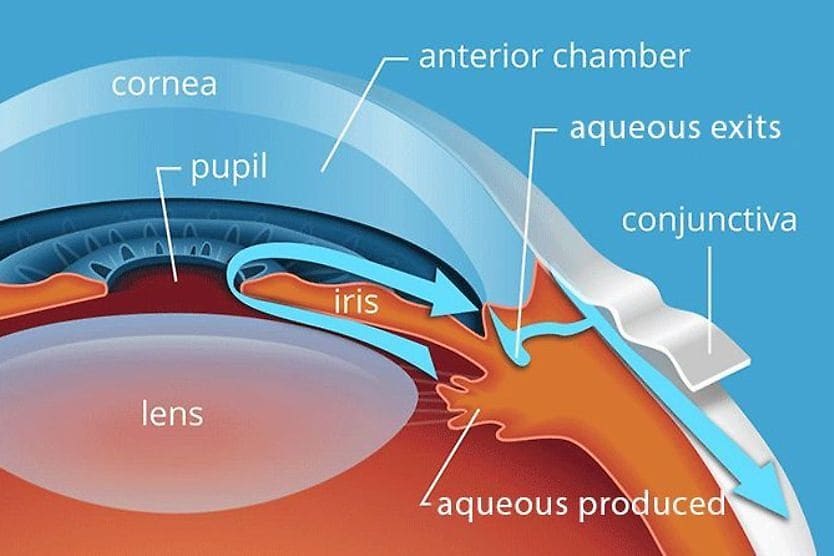
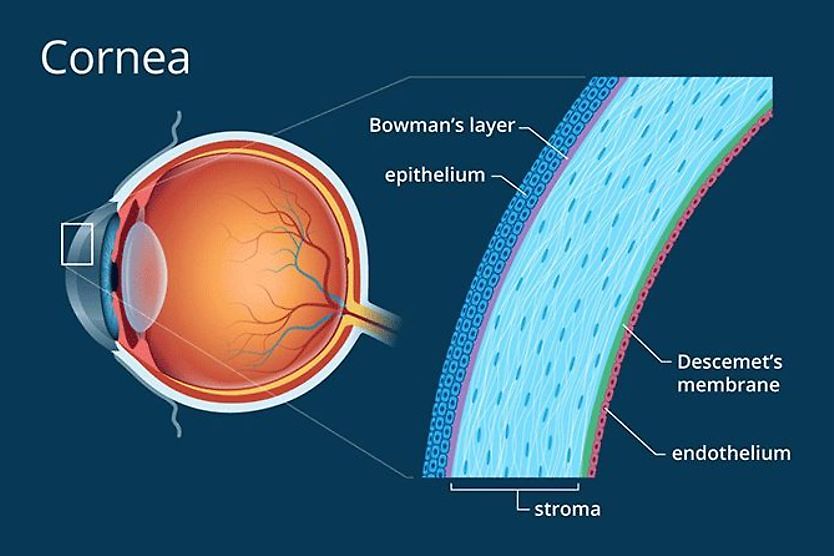
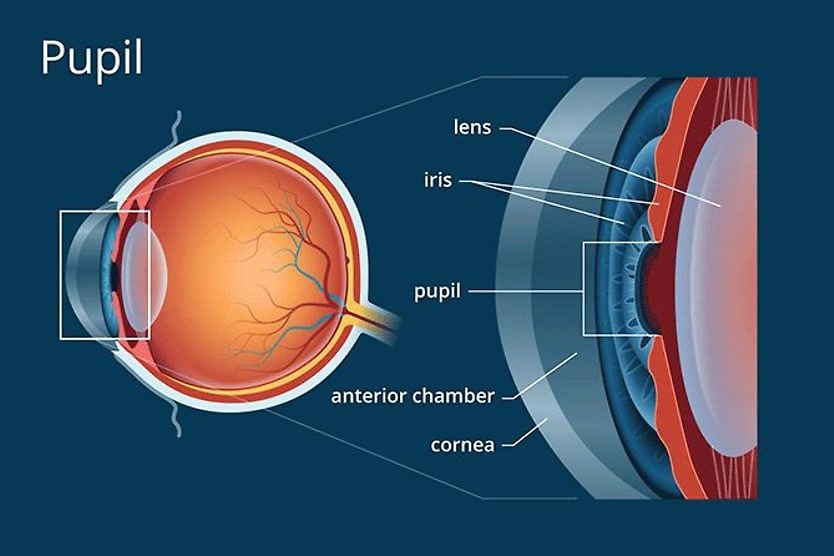
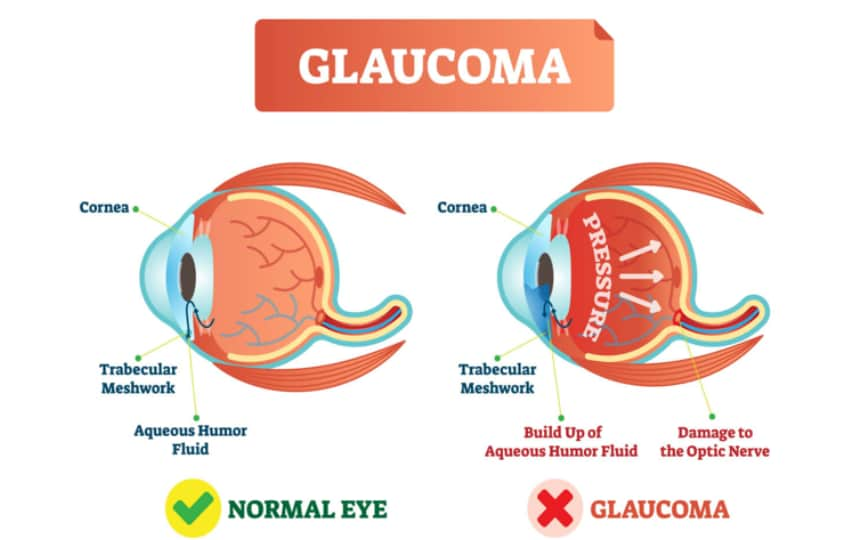
The trabecular meshwork is a 360-degree spongy structure located at the angle where the iris and the base of the cornea meet. It regulates eye pressure by draining aqueous humor, a fluid produced inside the eye that nourishes the cornea and lens.
To maintain normal eye pressure — intraocular pressure (IOP) — the drainage of aqueous humor at the trabecular meshwork must be balanced with its production. IOP will rise to high levels if the trabecular meshwork is not draining properly. This can injure the optic nerve and lead to vision loss, causing a condition called glaucoma.
Trabecular meshwork function
The trabecular meshwork is the eye’s drainage system. It returns excess aqueous humor into the bloodstream so it does not build up in the eye. If the trabecular meshwork is not draining properly, the eye pressure will increase. This will cause damage to the nerve that connects the eye to the brain — the optic nerve.
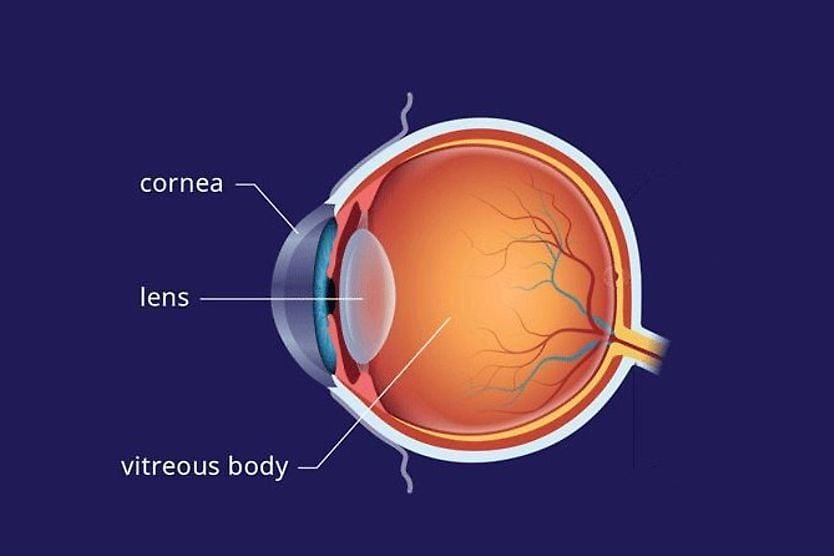
Aqueous humor is a plasma-like fluid that provides nutritional support to the eye’s structures that do not receive nourishment from blood vessels. This includes the lens and cornea. It also provides a balanced amount of pressure within the eye to maintain the eyeball’s shape and promote healthy function.
Trabecular meshwork anatomy
The trabecular meshwork is made of spongy tissue — a meshwork of tiny canals that drain most of the aqueous humor from the eye and direct it into the body’s blood circulation.
Once the aqueous humor drains through the trabecular meshwork, it flows through a small area called Schlemm’s canal, through channels that collect the fluid, and finally into veins, where it flows back into the bloodstream.
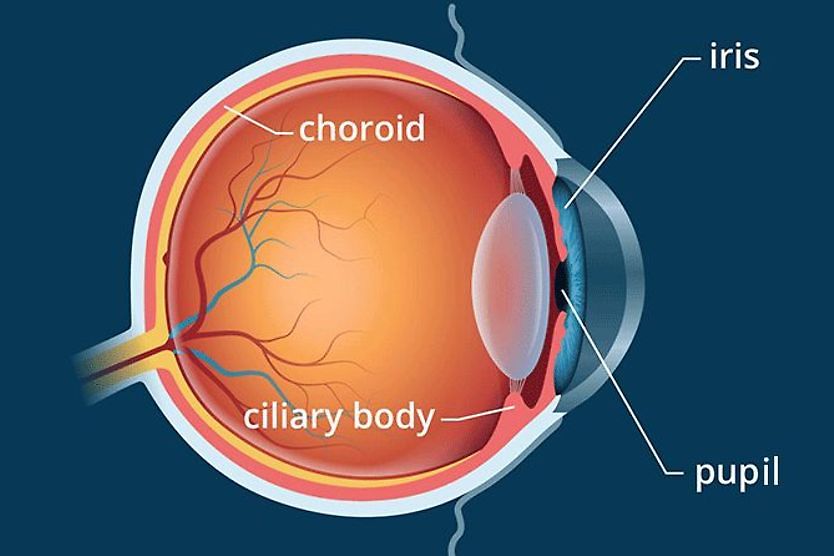
The location of the trabecular meshwork is known as the “angle.” This is the junction of the iris (colored part of the eye) and the cornea (clear, dome-shaped tissue at the front of the eye).
Gonioscopy
Eye doctors perform gonioscopy with a special mirrored lens to visualize the angle and evaluate the trabecular meshwork. The angle sits around the corner inside the eye, and the use of lens mirrors is necessary to see the anatomy of the angle and trabecular meshwork. This exam only takes a few minutes.
The procedure for gonioscopy is as follows:
- A drop of anesthetic is applied to numb the eye.
- A clear gel may be placed on the eye to make the lens more comfortable.
- The chin is placed in the chin rest of a slit-lamp microscope, an instrument used to look at the outside and inside of your eyes.
- You will be asked to look up so the special lens with mirrors can be placed on the eye's surface.
- You will be asked to look straight ahead, and a beam of light will be used to see the trabecular meshwork and drainage angle.
Importance of eye fluid drainage
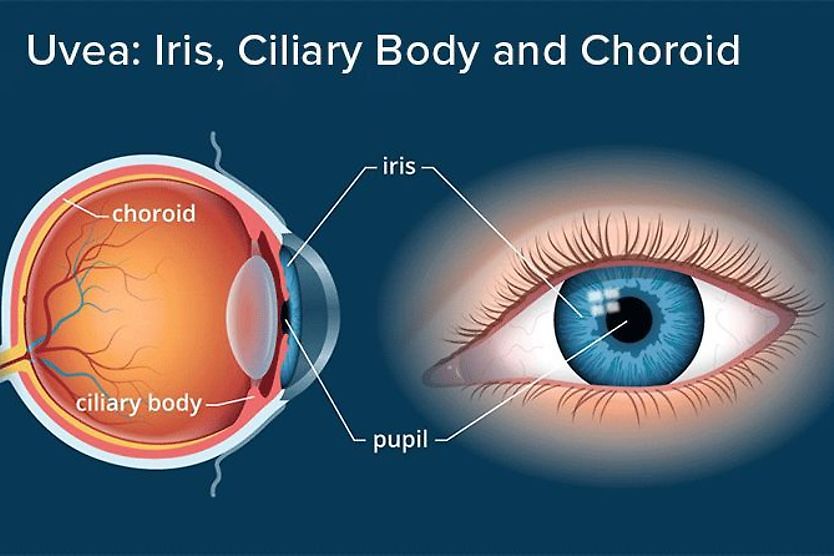
Aqueous humor is constantly refreshed through the inflow of new aqueous humor. This process involves the production of aqueous by the ciliary processes — a part of the ciliary body that is an extension of the iris.
The aqueous humor flows through the pupil and provides nutritional support to the eye’s lens and cornea. Most of the aqueous leaves the eye (outflow) through the trabecular meshwork and drains into the aqueous veins.
If the trabecular meshwork is not draining properly, the eye pressure will increase. Increased pressure in the eye can damage the optic nerve and lead to progressive vision loss.
Conditions affecting the trabecular meshwork
If there is increased resistance to aqueous humor passing through the trabecular meshwork, open-angle glaucoma can result. Open-angle glaucoma is differentiated from closed-angle by the presence of an open angle where the iris and cornea meet (where the trabecular meshwork is found) rather than a closed or narrow angle.
Glaucoma causes changes to the optic nerve head, progressive loss of peripheral vision and eventual loss of the central visual field. In some cases of open-angle glaucoma, the trabecular meshwork functions properly, but the ciliary processes produce too much aqueous humor. In either case, most cases of glaucoma are believed to be caused by high IOP.
Trabecular meshwork and glaucoma
Most causes of open-angle glaucoma are thought to be due to reduced aqueous drainage caused by an improperly functioning trabecular meshwork. Several different mechanisms may cause increased resistance to aqueous flow through the trabecular meshwork. These include:
- Conditions that clog the trabecular meshwork (for example, pigment or red blood cells)
- Loss of trabecular endothelial cells
- Loss of trabecular endothelial cells’ ability to destroy foreign particles — known as “phagocytic activity”
- Loss of giant vacuoles (spaces that hold waste in a cell) in the cells that line the inner layer of Schlemm’s canal
- Diminished size and density of the pores in the wall of Schlemm’s canal
These mechanisms can lead to the accumulation of debris in the aqueous humor and clog the meshwork through which the aqueous drains.
Conditions that clog the trabecular meshwork
In open-angle glaucoma, some conditions can cause microscopic particles to lodge into the tissue of the trabecular meshwork, making it difficult for aqueous humor to exit the eye. This leads to increased IOP.
Conditions and factors that can clog the trabecular meshwork include:
- Pseudoexfoliation syndrome – This condition causes a build-up of small protein fibers that have flaked off of the lens and lodged in the trabecular meshwork.
- Lens proteins from cataract surgery – During cataract surgery, lens proteins produced as part of the surgery can land in the trabecular meshwork, clogging it.
- Pigmentary glaucoma or pigment dispersion syndrome – This secondary glaucoma results from pigment from the iris flaking off and lodging in the trabecular meshwork.
- Red blood cell accumulation – If there is an internal injury to the eye, red blood cells can stick in the trabecular meshwork.
- Melanomalytic glaucoma – Small particles from a tumor in the eye can clog the trabecular meshwork.
- Corticosteroids – Steroid therapy, particularly eye drops, can impair a trabecular endothelial cell’s ability to destroy foreign particles (phagocytic activity). This leads to the accumulation of debris in the aqueous humor and increases IOP.
Open-angle glaucoma versus closed-angle glaucoma
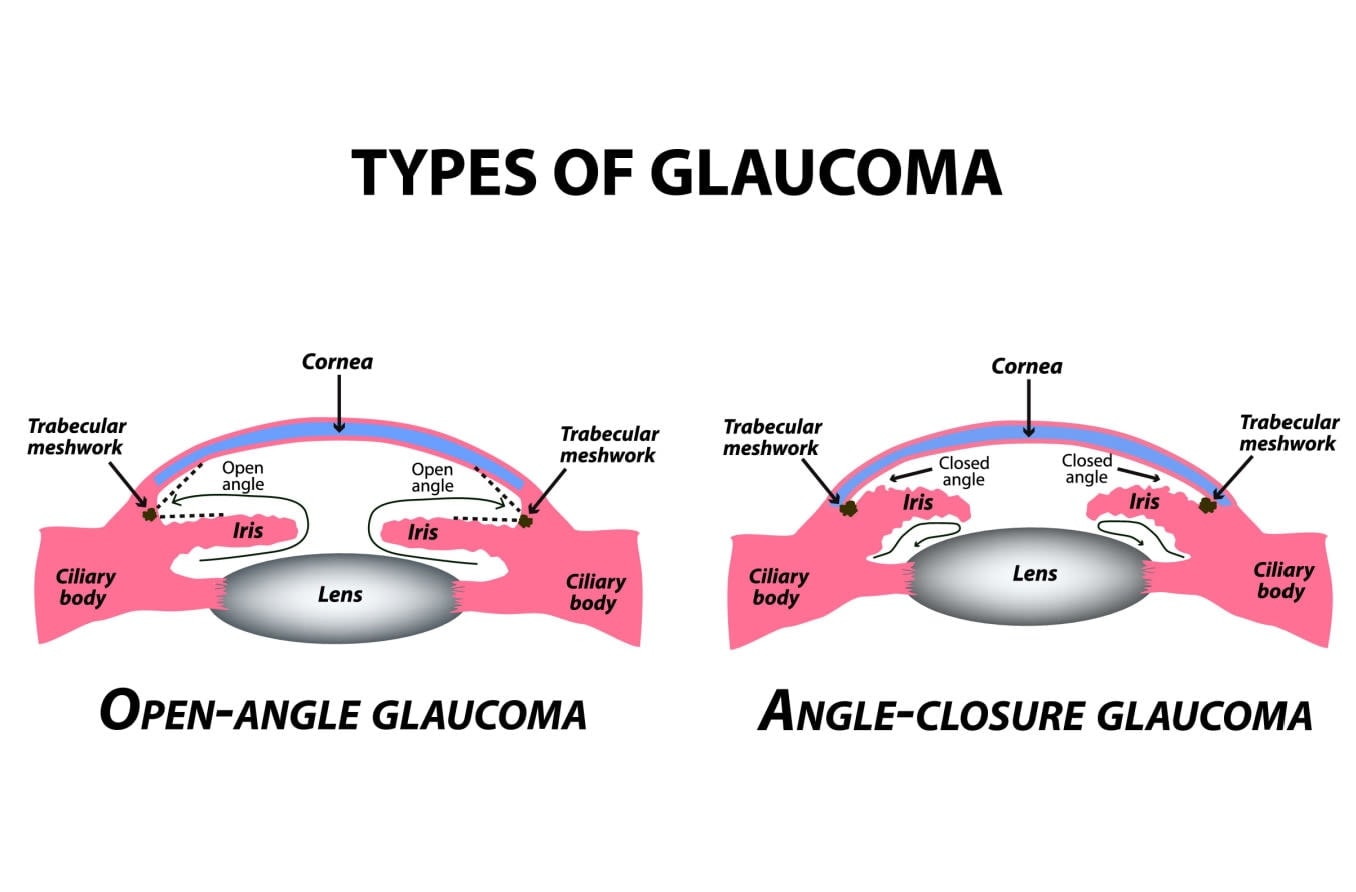
Closed-angle glaucoma and open-angle glaucoma can both cause vision loss, although the mechanism is different. Closed-angle glaucoma results from the angle between the iris and cornea being so narrow that the fluid cannot properly reach the trabecular meshwork and drain out of the eye. Acute glaucoma occurs when a narrow angle closes, and the aqueous cannot drain at all, causing intraocular pressure to rise to very high levels rapidly.
READ MORE: Glaucoma: Types, causes, symptoms and treatment
Maintaining healthy trabecular meshwork
One theory is that as we age, we lose trabecular cells, which play a role in the healthy functioning of the trabecular meshwork. This may be a reason that the risk for glaucoma increases as we get older.
Maintaining a healthy body will benefit the eyes overall, which could be beneficial in maintaining the trabecular cells of the trabecular meshwork as we age.
Some glaucoma surgery options also exist to improve the drainage of aqueous humor:
Selective Laser Trabeculoplasty (SLT)
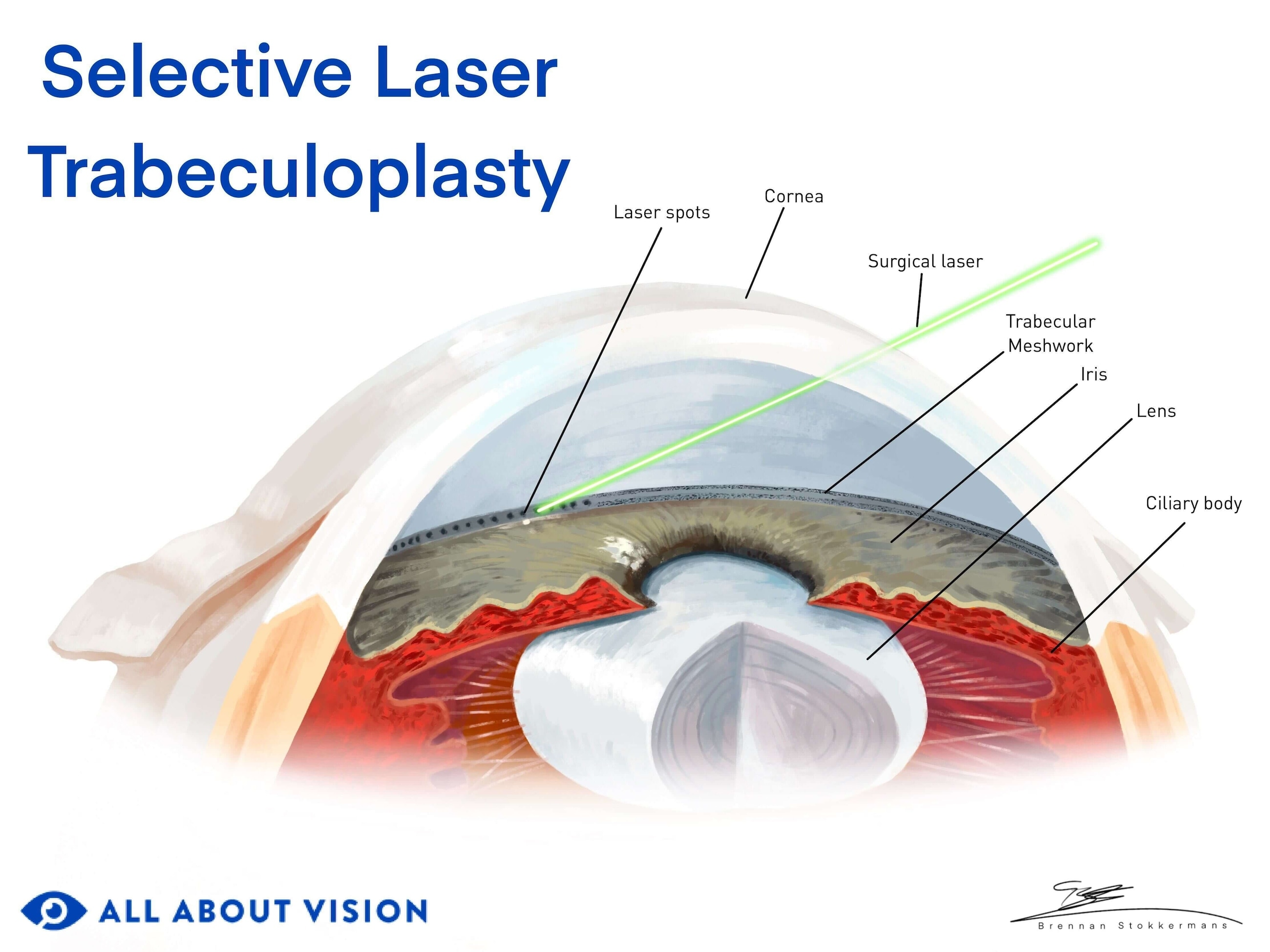
This surgery is performed on people with open-angle glaucoma, the most common type. The pressure usually increases slowly in this type of glaucoma. An eye doctor performs this procedure with a cold laser to increase the outflow of aqueous humor through the trabecular meshwork.
Using a cold laser (rather than a thermal laser) decreases the amount of scar tissue, allowing it to be a repeatable procedure. It is widely considered the first line of treatment for people with open-angle glaucoma. It is an in-office procedure, and usually, only numbing drops are required.
Argon Laser Trabeculoplasty (ALT)
This is another procedure used to treat open-angle glaucoma. The surgery is performed with a thermal laser instead of a cold laser. It is also an in-office procedure.
The objective of SLT and ALT surgery is to help maintain the trabecular meshwork’s ability to drain aqueous humor out of the eye. The laser can make drainage more effective, lowering eye pressure within the next few months. Unlike SLT, ALT is typically a one-time procedure depending on how much of the drainage system received laser treatment (180 degrees vs. 360 degrees).
The procedure for SLT and ALT is as follows:
- An eye drop that helps prevent a rise in eye pressure after the procedure is placed in the eye (typically, this is apraclonidine).
- A drop of anesthetic is applied to numb the eye.
- A clear gel is placed on the eye so that a special lens can be placed on it.
- A lens is placed on the eye to help focus the laser on the trabecular meshwork. It also prevents the eye from blinking and keeps it still during the procedure.
- A laser will be focused on the trabecular meshwork in a series of pulses. Clicks and flashes of light may occur while the laser is used.
The procedure is essentially painless. The doctor may slowly rotate the lens as they treat different areas of the trabecular meshwork. The procedure typically takes five to 10 minutes.
When the laser treatment is complete, the lens will be removed, although the gel may take about an hour to clear from the eyes. Your IOP will be checked to ensure that it has not risen too much. You may be given anti-inflammatory eye drops for several days and will be seen one to six weeks after the procedure.
Trabeculectomy
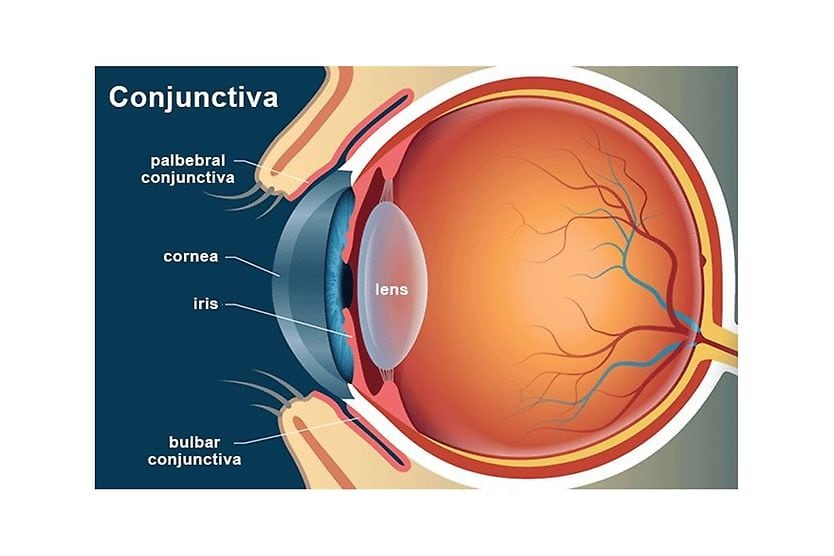
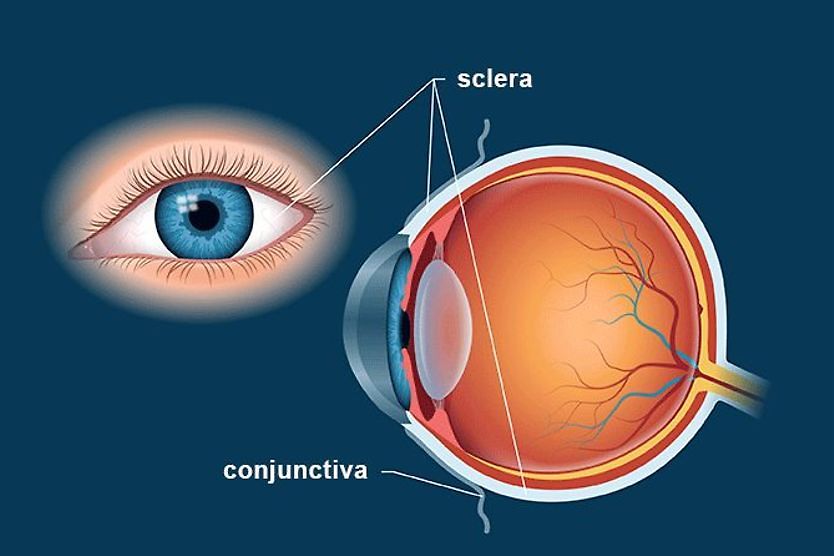
A trabeculectomy is a filtration surgery that creates an opening under the eyelid in the whites of the eye (the sclera) to provide a new pathway for excess aqueous humor to drain. The conjunctiva (a clear, thin tissue that covers the sclera) covers the opening, creating a “bleb” on the sclera.
This surgery is performed in a hospital and is typically recommended when laser surgery is ineffective at increasing the drainage function of the trabecular meshwork. It is more intensive and requires an incision. The surgery lasts about one hour, and you can usually go home on the same day.
Micro-invasive glaucoma surgery (MIGS)
MIGS is a newer procedure that is helpful for individuals with mild to moderate glaucoma who find it difficult to use eye drops regularly or if their IOP is not controlled by eye drops or laser surgery.
There are many types of MIGS. Some of these types address restricted drainage of aqueous humor through the trabecular meshwork and through Schlemm’s canal.
MIGS procedures that work on the trabecular meshwork or Schlemm’s canal include:
- Placing a stent in the trabecular meshwork to bypass it so that aqueous humor will flow directly into Schlemm’s canal.
- Goniotomy or trabeculotomy, which involves the removal of trabecular meshwork tissue so there is improved flow into Schlemm’s canal. This is done with a surgical incision or excision.
- Dilation of Schlemm’s canal to improve aqueous humor outflow.
Other approaches for MIGS include increasing the outflow of aqueous by alternate pathways and decreasing the amount of aqueous humor produced.
READ MORE: Types of eye surgery and the conditions they treat
When to see a doctor
Comprehensive, routine eye exams are important for everyone. Glaucoma is the leading cause of irreversible blindness worldwide. An estimated 76 million people worldwide are affected by it, and doctors believe this will increase to nearly 112 million in 2040.
Open-angle glaucoma, which can occur when the trabecular meshwork is not draining properly, is the most common form — accounting for up to 85% to 95% of cases. There are often no early symptoms, and nearly half of people with glaucoma don’t know they have the condition.
There is no cure for glaucoma at this time. But if it is caught early through routine eye exams, vision loss can be prevented.