Third nerve palsy (oculomotor nerve palsy)

What is third nerve palsy?
Third cranial nerve palsy occurs when CN III loses function. This results in symptoms such as misaligned eyes, double vision, drooping eyelid or enlarged pupil. It can be present at birth or be the result of an injury, disease or infection. A sudden onset of symptoms is a medical emergency.
The third cranial nerve is the oculomotor nerve (CN III). It is one of 12 pairs of nerves that lead from the brain to the face, head or torso. CN III carries signals from the brain to most of the muscles that move the eye. It also carries the nerve fibers that make the pupil smaller and lift the eyelid.
Each cranial nerve pair innervates the left and right sides of the face. Due to this, only one eye is usually affected by third nerve palsy.
If someone is experiencing symptoms of third nerve palsy, it is important that they see a doctor as soon as possible, particularly if the pupil is dilated. Imaging tests will need to be ordered to check for an aneurysm, herniation or tumor in the brain compressing the nerve.
Third nerve palsy symptoms
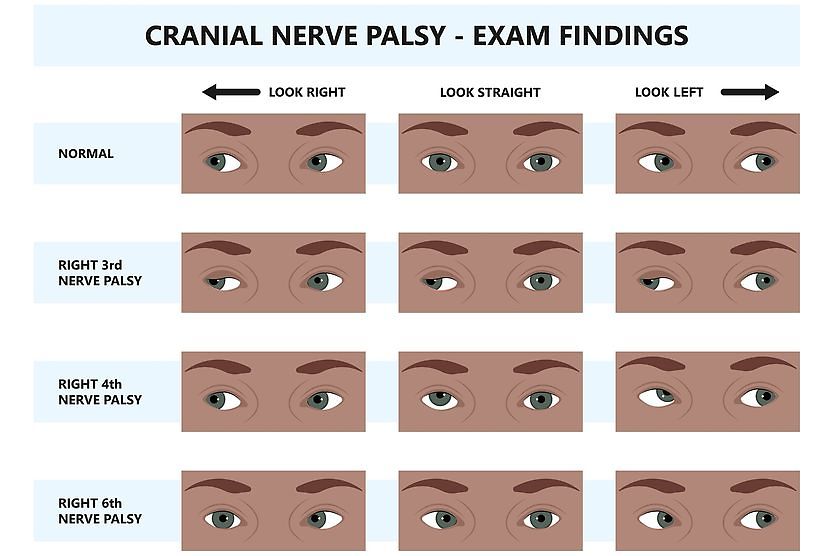
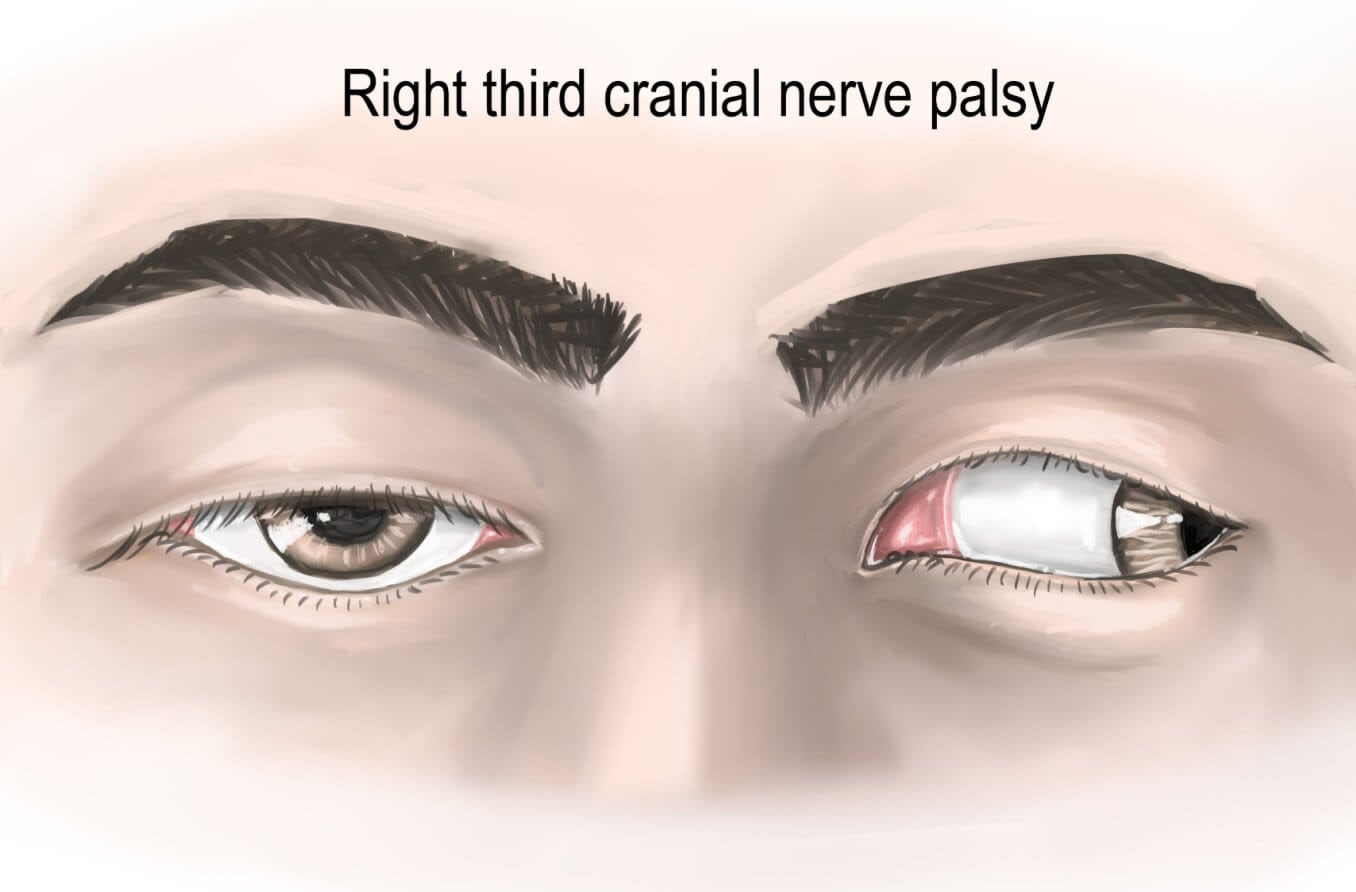
Symptoms of third nerve palsy are double vision,droopy eyelids, dilated pupil and a down-and-out gaze.
Understanding the functions of the third cranial nerve will make it easier to understand what happens when it is not functioning properly. The prefix “oculo-” means relating to the eyes or vision. The root word “-motor” means to move. The oculomotor nerve is a motor nerve that causes the eyes to move.
The third cranial nerve has two types of fibers that are bundled on the inner and outer sections of the nerve. Voluntary motor fibers run on the inside of the nerve, and involuntary fibers run on the outside of the nerve. Being aware of which types of nerve fiber bundles run on the outside and inside of CN III can help to understand why specific symptoms of cranial nerve palsy occur.
It is important to note that CN III palsy can be partial, and only some of the signs and symptoms may be present. Depending on the underlying cause, symptoms such as headache or drowsiness may also occur.
Symptoms of third nerve palsy caused by injury to inner nerve fibers
Conditions that damage the inner nerve fibers of the third cranial nerve will result in eye misalignment — strabismus — and impair the ability to raise the upper lid.
The nerve fibers that run on the inner portion of cranial nerve III control eye muscles that move the eyeball up, down and in, plus the muscle that lifts the upper eyelid.
The voluntary muscles controlled by the inner nerve fibers of CN III are:
- Superior rectus (SR) muscle – Moves the eye up while gazing straight ahead
- Medial rectus (MR) muscle – Moves the eye toward the nose while gazing straight ahead
- Inferior rectus (IR) muscle – Moves the eye down while gazing straight ahead
- Inferior oblique (IO) muscle – Moves the eye up while looking toward the nose
- Levator palpebrae superioris (LPS) muscle – Raises the upper eyelid
Symptoms of third nerve palsy caused by damage to the inner nerve fibers include:
- Down-and-out gaze – The affected eye will drift away from its normal position because it is being pulled in the direction of the opposing muscle.
- Double vision (diplopia) – This is the result of the eyes becoming misaligned. The affected eye sees an image from a down-and-out gaze, while the other eye looks straight ahead and sees a different image, leading to double vision (diplopia).
- Droopy eyelid (ptosis) – The LPS muscle does not work properly, causing the eyelid to droop.
The SR, MR, IR and IO muscles are responsible for coordinated eye movements. An individual with third nerve palsy will have difficulty fixating on objects and tracking them.
Note that damage to the inner nerve fibers does not affect the pupil.
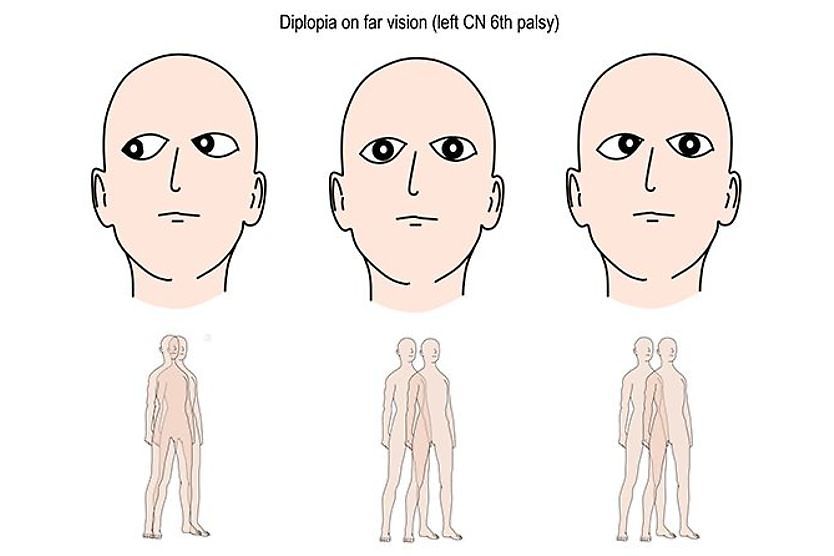
An interesting fact is that double vision does not occur in outward gaze. This is because the muscle that is responsible for this movement is not innervated by CN III but by CN VI.
Symptoms of third nerve palsy caused by compression of outer nerve fibers
Conditions that compress the outer nerve fibers of the third cranial nerve will affect the pupil and the eye’s ability to focus.
The nerve fibers that run on the outer section of cranial nerve III supply muscles that are part of the parasympathetic nervous system. The parasympathetic nervous system controls functions when the body is in a resting state. These fibers control involuntary processes.
The muscles controlled by the outer nerve fibers of CN III are:
- Sphincter pupillae – A muscle that is located in the colored part of the eye and responsible for constricting the pupil (making it smaller).
- Ciliary muscle – A muscle that surrounds the eye’s lens and causes it to become more spherical in shape, allowing close-up objects to be in focus.
Symptoms of third nerve palsy caused by compression of outer nerve fibers include:
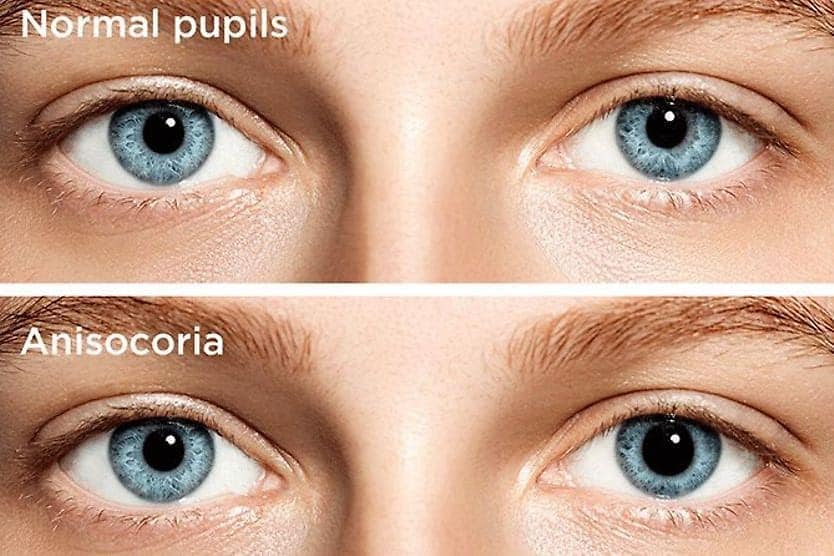
- Enlarged pupil – This occurs because the outer fibers of CN III cannot send signals to the sphincter pupillae muscle, which is responsible for making the pupil smaller. As a result, the pupil dilates (sometimes called a “blown pupil”), leading to anisocoria (pupils that are unequal in size).
- Inability to focus up close – This occurs because the ciliary muscle is no longer receiving signals to contract. So, the lens is unable to focus incoming light rays from close-up objects.
Causes of third nerve palsy
Some individuals are born with a third nerve palsy (congenital). It can also be acquired due to injury or disease.
Conditions that damage the inner fibers of CN III
Some diseases can, over time, injure the small blood vessels that supply cranial nerve III, limiting blood flow to the nerve. When blood flow to CN III is restricted, the inner nerve fibers can no longer effectively transmit signals to the muscles responsible for eye movement and lid elevation. Although the inner fibers are affected, the outer fibers may be spared, and the pupil remains normal.
The conditions that damage the inner fibers of CN III include:
- Diabetes
- High blood pressure
- Inflammatory diseases
Conditions that damage the outer fibers of CN III
Some conditions compress the outer fibers of CN III. This can damage fibers that control the sphincter pupillae muscle and ciliary muscle, resulting in a dilated or “blown pupil” and an inability to accommodate.
The conditions that damage the outer fibers of CN III include:
- Aneurysm – A bulge in a blood vessel in the brain.
- Herniation – Increased pressure inside of the skull that shifts brain tissue. The herniation is often due to injury, stroke, bleeding a tumor or swelling.
- Meningitis – Inflammation of the meninges, a membrane that surrounds and protects the brain and spinal cord (for example, due to tuberculosis).
- Tumor – An abnormal mass located in the brain or brainstem.
- Injury – Trauma that results in damage to CN III along its path from the brain to the eye.
SEE RELATED: 7th cranial nerve
Third nerve palsy in children
A third cranial nerve palsy is rare in children. Young children with cranial third nerve palsy cannot express that they are experiencing double vision. However, parents will typically notice the other signs and symptoms.
Symptoms
If poor vision goes undetected in young children, they can be at risk for a condition called amblyopia (“lazy eye”). This condition can be treated if detected early. But it can result in life-long decreased visual acuity and depth perception if detected too late.
The symptoms of third nerve palsy in children include:
- Double vision
- Misaligned eyes
- Droopy eyelid
- Enlarged pupil
If the eyelid droops over the pupil, a child may not have double vision because they are only seeing with the unaffected eye. A child may also adopt an abnormal head tilt to compensate for double vision.
Causes
Up to half of the cases of third nerve palsy in kids are congenital, which means the palsy was present at birth. Congenital third nerve palsy is not a life-threatening condition. But it is important that the child have a thorough medical exam to ensure that there are no other medical issues.
Additional causes of acquired third nerve palsy in children include:
- Injury
- Inflammation
- Damage to blood vessels
- Infection (uncommon)
- Tumor (uncommon)
Treatment
In addition to surgical treatment and optical correction, vision therapy may be recommended to help the eyes learn to work together. If a child is at risk for amblyopia, the normal eye is typically covered with a patch — sometimes for several years.
Third nerve palsy diagnosis
A comprehensive eye exam, neurological exam, laboratory tests and imaging may be needed to diagnose the cause of third cranial nerve palsy.
If the pupil is involved, a doctor may order imaging tests to determine the cause of compression to the outer nerve fibers of CN III. These tests may include:
- MRI – Magnetic resonance imaging that produces three-dimensional images of the brain
- CT angiography – Computed tomography angiography, which produces images of tissues and blood vessels if an aneurysm is suspected
If the pupil is not involved, a doctor may order the following tests to determine whether there is an underlying disease, such as diabetes and hypertension, or a disease that is causing inflammation:
- HbA1C – Measures average blood sugar levels over the past three months
- CBC – Complete blood count, provides a general analysis of overall health
- ESR – Erythrocyte sedimentation rate, indicates inflammation in the body
- BP – Measurement of blood pressure
READ MORE: 15 ways heart disease affects eye health
Third nerve palsy treatment and prognosis
Treatment for third nerve palsy depends on the underlying cause. In cases involving a medical emergency, such as an aneurysm, brain herniation or tumor, urgent medical or surgical intervention may be needed.
When third nerve palsy is related to a condition such as diabetes or high blood pressure, treatment typically focuses on managing that condition first. In non-emergency cases, eye doctors often take a watchful approach, monitoring the patient over several months to see whether the palsy resolves on its own. Many people see improvement within a month, and most can recover fully within three months.
In the meantime, symptoms such as double vision can often be managed with prism eyeglasses or an eye patch. If symptoms have not improved after six months or more, an eye doctor may recommend surgery to help align the eyes or lift a drooping eyelid.
When to see a doctor
It is important to seek urgent medical care if you notice a sudden development of double vision, changes in vision, eye misalignment or an abnormally enlarged pupil. In particular, an abnormally enlarged pupil in one eye may indicate bleeding in the brain, an aneurysm or a tumor — all life-threatening conditions.
Cranial nerve three palsy may be a medical emergency and should be treated as such.