What’s new with age-related macular degeneration

What a difference a few years make. Ten years ago, a patient diagnosed with age-related macular degeneration (AMD) had limited treatment options. Whether they had dry AMD, a more common, slower-progressing form of the disease, or wet AMD, which can cause sudden, rapid vision loss, the prognosis was grim.
Anecdotes posted in online patient support groups, while not clinically verified, illustrate the difference between then and now. As recently as 2022, one person shared that their macular degeneration had worsened to the point that they had to stop driving. They sold their car and cancelled their insurance, relying instead on friends for rides and support.
Just four years later, it appears the mood may have shifted a bit. Another person posted about their second photobiomodulation session (known as PBM — a form of red light therapy) of nine treatments. After an evaluation (dilated and tested) the outcome appeared encouraging: their vision seemed to have stabilized, even improved, if just a little.
Since AMD often goes undetected in its early stages, many people received a diagnosis after the disease had already done significant damage. Eye doctors caution that while outcomes vary, patients should be aware that wet AMD can lead to significant central vision loss over time.
Indeed, AMD is still the leading cause of partial and central vision loss in American adults over 50, and there is an avalanche of new treatments, technologies and research related to the disease. This work is slowly changing what a diagnosis means for the 20 million Americans who have AMD. These new advancements are altering what patients can expect of their long-term vision and eye health.
Understanding dry and wet AMD
Age-related macular degeneration is a disease that develops and presents in many ways. “Some patients have AMD and it progresses so slowly and impacts their vision so minimally that they don’t even know that they have it,” said Joseph N. Martel, MD, an associate professor of ophthalmology at the University of Pittsburgh and director of the retina service at UPMC Vision Institute. “And then there are other patients who have severe forms that may progress faster, where they lose basically all of the fine details in vision.”
Dry age-related macular degeneration is the most common type of the disease. It affects about 90% of all AMD patients, according to the American Macular Degeneration Foundation. Both types of AMD impact the macula, a part of the retina responsible for sharp, detailed central vision and color vision.
With dry AMD, the macula gets thinner over time. This thinning, called atrophy, is also characterized by tiny drusen (metabolic waste) that build up in the retina. This stage may take years or even decades to develop.
Wet AMD can develop after someone is diagnosed with dry AMD, although some people could get wet AMD on its own. Usually aggressive, wet AMD happens when abnormal blood vessels grow under and within the retina. When blood and fluid leak into the tiny space, scar tissue can form. In the worst-case scenario, wet AMD may cause rapid and significant vision loss.
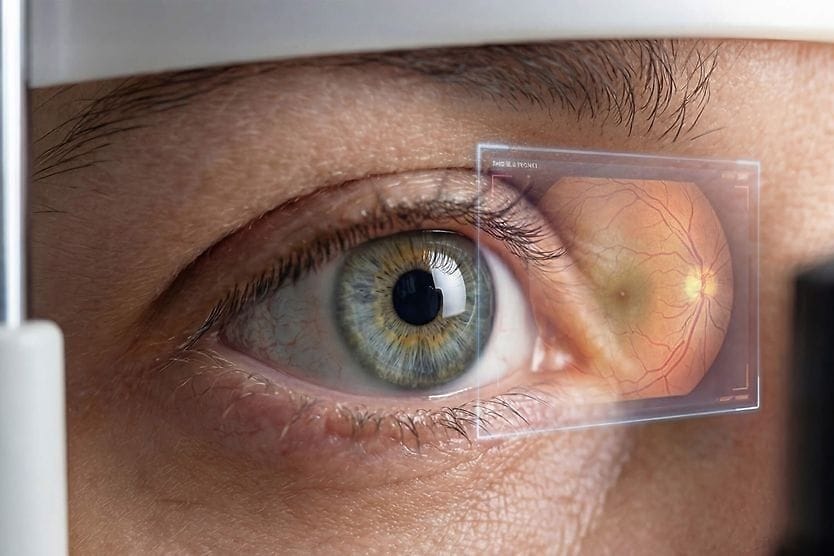
In both types of AMD, the symptoms are similar. Patients, usually over 50, might notice a little dark or shadowed spot in their vision, waviness, or some blind spots. Eye doctors perform tests for AMD, including vision testing and a non-invasive imaging test called optical coherence tomography angiography (OCT/OCTA).
“The OCT image is sort of like an X-ray of the retina,” Dr. Martel said. “It allows us to look at the microscopic layers of the macular retina and look specifically for degenerative changes — presence of drusen, presence of fluids.”
Even a few years ago, once eye doctors made a diagnosis, prognosis could go either way, Daniel Palanker, PhD, a professor of ophthalmology at Stanford University explained.
“There were no real treatments,” he said. “This is a disease that leads to loss of photoreceptors, and there was no way to restore photoreceptors.”
Treatments for macular degeneration
For a long time, patients had few options for treating their disease. Doctors recommended supplements for both wet and dry forms of AMD. Laser treatments were offered for wet AMD. They also told patients to stop smoking and suggested assistive devices such as magnifying glasses to help them read. These steps could — and still can — help, but there were limited research-backed clinical treatments shown to slow or stop the disease’s progression.
Then just over 20 years ago, one of the most important moments in AMD treatment happened when anti-vascular endothelial growth factor (anti-VEGF) drugs were introduced. These injections were designed to slow the abnormal blood vessel growth that could lead to wet AMD.
Rahul Khurana, MD, clinical associate professor in ophthalmology at UCSF Medical Center and a retina specialist, said this class of drugs has “really revolutionized our treatment” for AMD patients. “The last 15 to 20 years with these anti-VEGF drugs, we've had a lot better outcomes. I do have many patients who can still read, drive and are very active, which is amazing,” he explained.
Treatment options for wet AMD continue to expand with the second-generation anti-VEGF drugs. A higher-dose version of aflibercept was approved to allow longer intervals between injections while maintaining visual outcomes comparable to standard dosing. Faricimab offers a similar advantage, with some patients able to extend treatment intervals up to every 16 weeks. A refillable implant was approved in 2024 that continuously delivers ranibizumab into the eye provides another option for patients seeking to reduce the frequency of in-office injections.
Dry AMD treatments are harder to find, according to John Hulleman, PhD, associate professor in the basic science division at the University of Minnesota and the Larson Endowed Chair for Macular Degeneration. “This is likely due to it being an inherently more complex form of the disease,” he explained.
Still, there are options. In 2023, the FDA approved the first-ever treatments for geographic atrophy (GA), the advanced stage of dry AMD. Pegcetacoplan and avacincaptad pegol target the complement pathway of the immune system, which is linked to AMD risk. These drugs have been shown to slow the expansion of GA-related retinal damage, marking an important first step in treating a condition that was previously untreatable.
Another new option for dry AMD is a treatment authorized by the FDA in late 2024. It uses low-level red light therapy, a technique called photobiomodulation (PBM). "It stimulates mitochondrial function," Dr. Martel explained. Mitochondria are the powerhouses of cells, giving them energy and contributing to cell healing and growth.
Those patients who have already lost some vision may benefit from Dr. Palanker's work. He and his team at Stanford have developed an implanted chip that is inserted under the damaged retina. The chip is thinner than a strand of human hair and works much like a solar panel would, turning light into electrical signals. Paired with augmented reality glasses, some people could read again.
“Currently we have about 45 patients implanted,” Dr. Palanker said. “The average improvement in visual acuity compared to baseline was five lines on a vision chart.” The treatment is expected to be approved in Europe as early as summer 2026, with FDA approval still in progress. More work needs to be done so patients could see objects such as faces and other details.
What comes next: Future AMD treatments
Researchers are investigating new therapies in the pipeline too. For instance, scientists at the National Institutes of Health have developed a digital replica of retinal pigment epithelial (RPE) cells, which can be damaged or destroyed when someone has AMD. They are using artificial intelligence to try and understand how AMD affects the RPE cells to find a way to address the disease at its root.
There are novel diagnosis tools too, according to Dr. Hulleman. “The most significant diagnosis advancement is the use of delayed dark adaptation assessment for the preventive detection of early and intermediate AMD. I believe that this is the best test so far to identify visual problems at a very beginning stage,” he said. It’s important to diagnose early so doctors can treat the disease when it starts, as opposed to when patients have symptoms and damage to the eye, he said.
Another group of treatments in development works a bit differently than anti-VEGF drugs. These medications are called tyrosine kinase inhibitors (TKIs). They are designed to block abnormal blood vessel growth from inside the cells of the retina rather than outside. Two TKIs currently being studied in late-stage trials for wet AMD are called axitinib and vorolanib. Both would be delivered as a single in-office injection using a tiny dissolvable implant that slowly releases the drug over time, with the goal of maintaining vision while reducing the need for frequent injections.
In addition, scientists are exploring gene therapy as a way to treat AMD. Instead of requiring frequent injections, these experimental therapies deliver genetic instructions that prompt cells in the retina to produce their own anti-VEGF proteins continuously. Several gene therapies for wet AMD are currently in clinical trials, each using different delivery methods and targeting slightly different pathways, with the goal of reducing or eliminating the need for ongoing injections.
“Using these treatments is not as far out as you think,” said Dr. Khurana. “We actually have some really exciting studies looking at gene therapy for macular degeneration as a way of delivering the medicine,” he added.
According to Dr. Khurana, current treatments require that people get regular injections either every month or every three months. The idea behind gene and TKI therapies is the potential to reduce or eliminate the need for frequent injections. This could make treatment easier to maintain and possibly help slow the progression of the disease.
Looking ahead, with hope
This research is important because, despite the spate of new treatments, there is still no cure for either type of AMD. “Even though there’s been progress over the last decade and probably much more to come, there’s unfortunately no cure for macular degeneration,” Dr. Martel said. “Many of these treatments are designed to slow down the progression.”
In the meantime, Dr. Martel says it’s important to have an eye care professional and tell them about any changes you see, even if they seem unimportant. “If you have risk factors for macular degeneration like family history, smoking history, or any vision changes like distortion, a spot in the vision or reduction in overall clarity, those are symptoms that should prompt you to see an eye doctor,” he said. “Particularly if you’re over the age of 60.”
With an early diagnosis, eye doctors can use existing treatments to potentially slow or halt the progression of AMD. Combined with future treatments, there’s definitely hope, Dr. Khurana said.
“There's a lot of excitement, a lot of clinical trials in the works, and a lot of reasons to be optimistic about the future,” he added.
NOTE: If you’re experiencing any symptoms described in this story, it’s important to consult an eye doctor for a comprehensive eye exam and discussion about individualized treatment options.