Eye stroke


What is an eye stroke?
“Eye stroke” is a lay term that describes a sudden loss of blood flow to the retina or optic nerve, two structures vital to vision and eye health. The condition often causes sudden, painless vision loss in one eye and is a medical emergency that requires time-sensitive care. In fact, the American Heart Association considers central retinal artery occlusion (CRAO) — the most well-known type of eye stroke — to be a form of acute ischemic stroke, the same category as a stroke in the brain.
Eye (ocular) strokes occur when the blood vessels serving the retina or optic nerve become blocked or when blood flow is disrupted, preventing these structures from receiving oxygen and nutrients. This can lead to vision loss, the severity of which depends on the extent and location of the blockage or restricted blood flow.
While the term “eye stroke” is commonly associated with central retinal artery occlusion (blockage), it can refer to the blockage of any blood vessel supporting the retina or optic nerve. Some experts use “eye stroke” to mean a specific type of retinal vascular occlusion (RVO). However, the terminology varies among specialists.
The main types of eye strokes include:
Central retinal artery occlusion (CRAO)
CRAO is the sudden blockage of blood flow to the retina through the central retinal artery, which is the main artery providing the retina with blood. It can cause the most damage out of all retinal artery occlusions, including sudden, severe vision loss in the affected eye.
Branch retinal artery occlusion (BRAO)
BRAO is a blockage in one of the smaller branch retinal arteries. These are branches of the central artery that supply blood to different parts of the retina. For this reason, BRAO may only affect one part of your vision.
Central retinal vein occlusion (CRVO)
The CRVO is the main vein that carries blood away from the retina. When this vein becomes blocked, the blood cannot drain properly and may pool in the vein. The blood can leak into the retinal tissues and cause them to swell, which can result in retinal damage that impacts most of your vision in the affected eye.
Branch retinal vein occlusion (BRVO)
BRVO is a blockage in one of the smaller branch retinal veins. These are branches of the central retinal vein that carry blood away from different parts of the retina. As a result, blood may collect in the veins, causing fluid leakage that leads to retinal damage. BRVO typically only affects part of your vision.
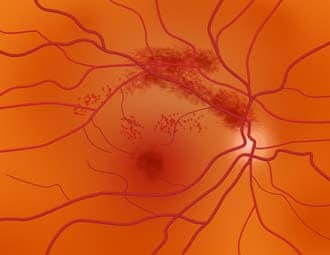
A branch retinal vein occlusion (BRVO) can develop from a blood clot.
Anterior ischemic optic neuropathy (AION)
Ischemic optic neuropathy is a lack of sufficient blood flow to the optic nerve. When it affects the front portion (the head) of the optic nerve or the optic disc, it’s referred to as anterior ischemic optic neuropathy (AION). The optic disc is where the optic nerve and the retina meet.
This condition is further categorized into two subtypes:
- Arteritic anterior ischemic neuropathy (AAION) – Involves the inflammation of blood vessels. The condition is the most common eye complication of giant cell arteritis (GCA).
- Nonarteritic anterior ischemic neuropathy (NAION) – Does not involve blood vessel inflammation. This is the more common form of AION.
Posterior ischemic optic neuropathy (PION)
Posterior ischemic optic neuropathy (PION) is a lack of blood flow to the rest of the optic nerve. PION is less common than AION and usually develops following a major surgery, such as those involving the heart, lungs, brain or spinal cord.
What are the symptoms of an eye stroke?
While symptoms of an ocular stroke can occur in both eyes, the majority of the cases only affect one eye. Pain is typically not a symptom.
Eye stroke symptoms can include:
- Sudden painless vision loss
- Sudden, significant blurring of vision
- Peripheral (side) vision loss
- Distorted vision
- Blind spots in your central or side vision
- Dark curtain or shadow in your vision
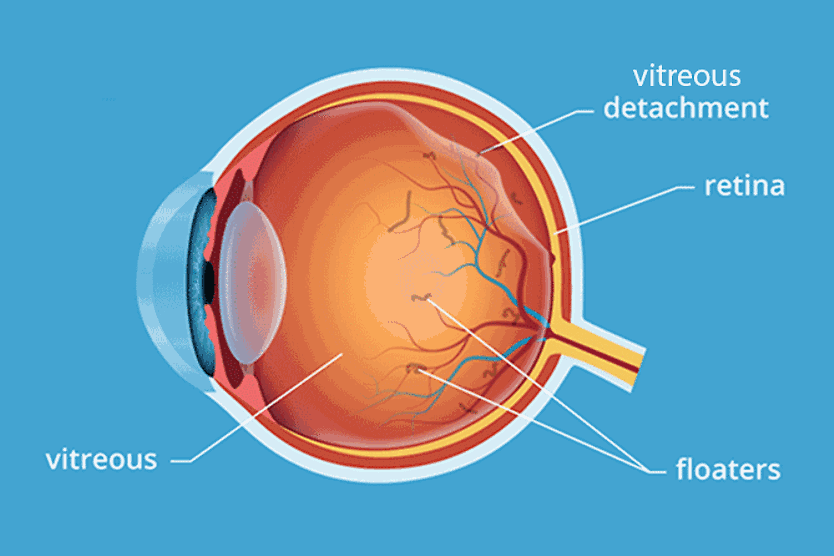
- Floaters and flashes of light
- Vision changes that start out small and then worsen over time
- Changes in visual color or contrast perception
- Light sensitivity
Many of these symptoms are red flags that require time-sensitive emergency care. Some cases have symptoms that typically come on suddenly, often within seconds to minutes. Even if your vision seems to improve on its own, the underlying event still requires immediate evaluation.
Brief episodes of vision loss that resolve (sometimes called amaurosis fugax) can be a warning sign of an impending eye stroke or brain stroke and should be treated as a medical emergency.
If you experience symptoms of a stroke in your eye, don’t wait to seek help. Go to your nearest hospital emergency room right away.
What causes an eye stroke?
Eye strokes occur when the retina or optic nerve does not receive a sufficient amount of blood. This can result from various vascular events, including:
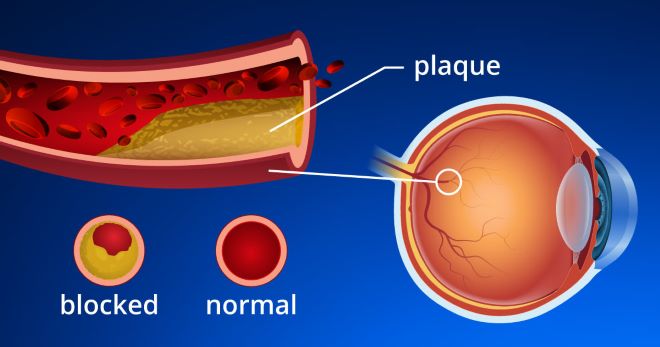
- Atherosclerosis – Narrowing of the arteries due to plaque buildup and hardening of the vessel walls.
- Embolism – Blockage of a blood vessel caused by a piece of arterial plaque, a blood clot or other substance that has broken off from another area of the body.
- Thrombosis – Blood vessel blockage that develops when the blood thickens and forms a clot.
- Vasculitis – Inflammation of the blood vessels, which can occur with inflammatory or autoimmune conditions, such as giant cell arteritis.
- Insufficient blood flow – Caused by factors such as blood loss or a drop in blood pressure.
Who is at risk for an eye stroke?
Certain systemic conditions and other factors can increase risk of an eye stroke, including:
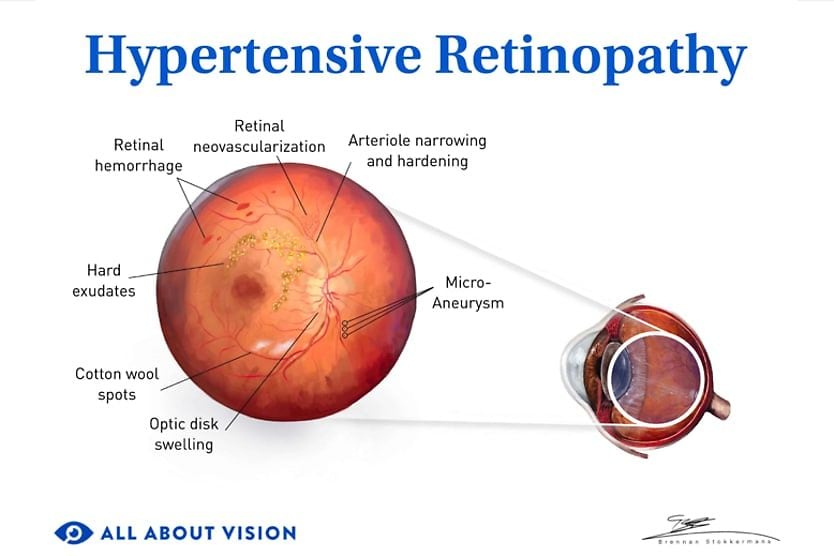
- High blood pressure
- Diabetes
- High cholesterol
- Cardiovascular disease
- Anticoagulant or blood-clotting disorders
- Prior transient ischemic attack (TIA)/stroke
- Glaucoma
- High intraocular pressure (IOP)
- Obesity
- Smoking
- Older age (age 50 or older for certain types of eye strokes)
In some people, an eye stroke may be the first sign of a vascular disease. Talk to your primary care physician and eye doctor to find out if there are ways to manage these risk factors. They may refer you to specialists like a cardiologist, neurologist or hematologist (a doctor who specializes in diseases of the blood).
How is an eye stroke diagnosed?
Eye strokes are diagnosed through a series of exams and imaging techniques. After reviewing your medical history and discussing your symptoms, your optometrist or ophthalmologist may perform one or more of the following:
- Comprehensive eye exam – Your eye doctor may test your visual acuity, visual fields, eye pressure and your pupil’s response to light. They may also use special drops to dilate (widen) your pupils so they can gain a clear view of your retina and optic nerve.
- Fluorescein angiography (FA) – A special dye is injected into your bloodstream (usually through a vein in your arm). Images of your eyes are taken as the dye travels through your ocular blood vessels, allowing your doctor to check for blockages.
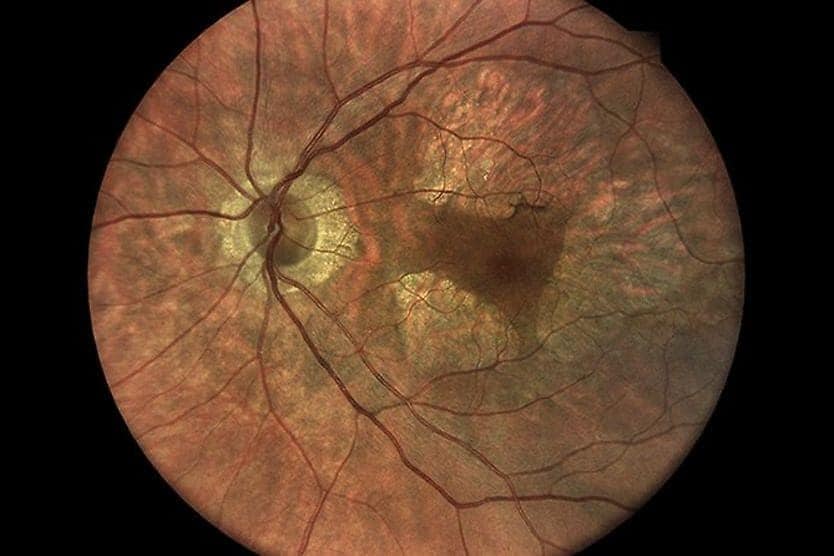
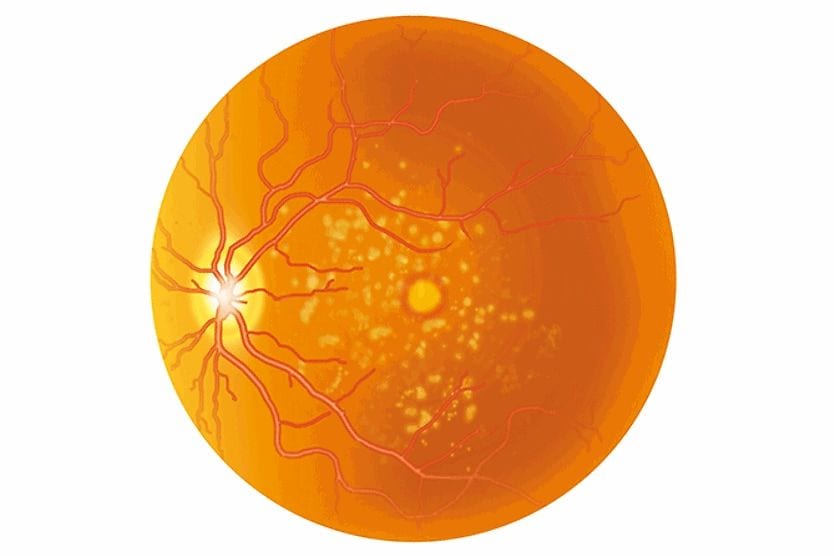
- Fundus photography – Your doctor may take pictures of the back of your eye (the fundus) to further examine the retina and optic nerve.
- Optical coherence tomography (OCT) – This non-invasive technique captures cross-sectional images of your retina and optic nerve. These pictures allow your doctor to evaluate the layers of these structures in greater detail.
- Optical coherence tomography angiography (OCTA) – Similar to OCT, this technique captures detailed images of the retinal blood vessels without the need to inject a special dye.
Because eye strokes can signal a broader vascular problem — and may occur alongside a brain stroke — additional testing is often recommended. This may include:
- Blood work – Inflammatory markers may be tested when giant cell arteritis is suspected. An eye stroke is a time-sensitive medical emergency.
- Brain imaging – An MRI of the brain may be performed to check for signs of stroke in the brain, which can occur alongside an eye stroke.
- Vascular imaging – Imaging of the carotid arteries and heart may be performed to look for a possible source of the blockage.
Diagnosing and treating an eye stroke usually involves a multidisciplinary health care team other than an eye doctor. Specialists may include:
- Neuro-ophthalmologist (an ophthalmologist who specializes in diagnosing and treating complex vision problems linked to the brain, nerves and nervous system)
- Radiologist
- Neurologist
What is the treatment for an eye stroke?
Like with a brain stroke, time-sensitive emergency care is required for a stroke affecting the eye. Quick treatment, usually within a few hours after the event, is imperative to reduce the extent of eye damage and permanent vision loss.
Treatment can vary based on the type of eye stroke that occurs, but it may include:
- Medication – Different types of medications may be prescribed to help break down the clot, control inflammation or lower intraocular pressure to improve blood flow within your eye.
- Eye massage – In some cases, doctors may apply firm pressure to your eye to help decrease intraocular pressure and loosen the blockage.
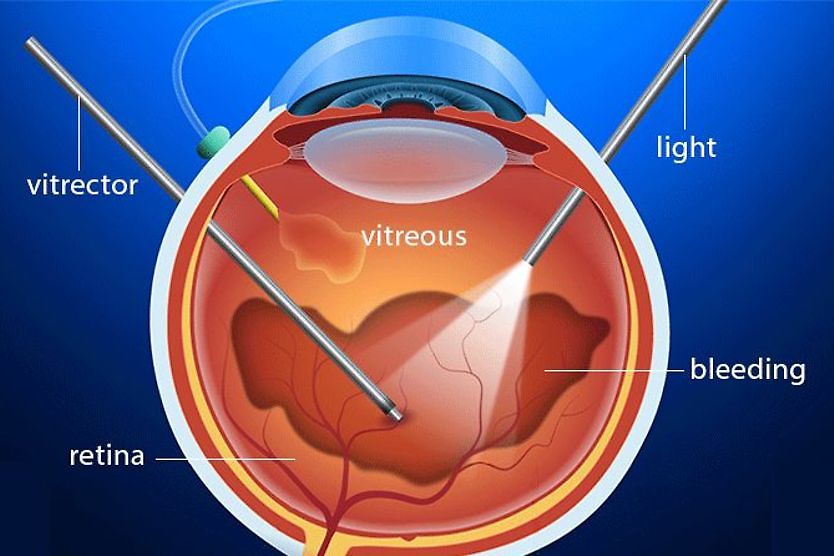
- Paracentesis – During this procedure, doctors in some cases may remove fluid from your eye to help lower internal pressure and increase blood flow.
- Hyperbaric oxygen therapy – This treatment, which involves breathing 100% oxygen inside a pressurized chamber, can be used in some CRAO cases to help reoxygenate the retina.
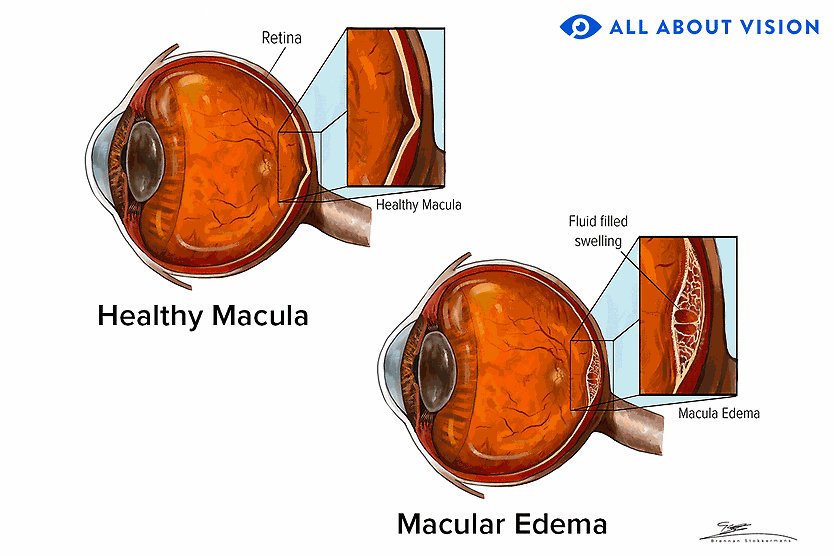
- Treatment of retinal complications – Following an RVO, complications such as macular swelling and the formation of abnormal new blood vessels are common. These may be managed with anti-VEGF (vascular endothelial growth factor) injections, corticosteroid injections or laser treatment.
Specifically for AAION caused by giant cell arteritis, doctors will prescribe urgent high-dose corticosteroid therapy that is typically started right away. This medication is used to help reduce the risk of significant vision loss in the unaffected eye. If the condition is untreated, it can rapidly threaten both eyes.
Overall treatment strategies may also involve addressing underlying systemic causes, such as high blood pressure, diabetes, heart disease or clotting problems. If permanent vision loss occurs, vision rehabilitation with low vision specialists may be recommended to help maximize your remaining vision.
How can you prevent an eye stroke?
While you may not be able to prevent an eye stroke from occurring, the following steps can help reduce your overall risk:
- Manage systemic risk factors – Work with your health care team to control health conditions, such as high blood pressure, diabetes and high cholesterol.
- Get regular comprehensive eye exams – It’s important to have your eyes and vision checked on a regular basis. If you’re at high-risk, your eye doctor may recommend more frequent visits to monitor your eye health and screen for eye stroke signs.
- Avoid or quit smoking – If you smoke, it is recommended to take steps to quit. Ask your health care provider for help with cessation if needed.
- Avoid excessive alcohol use – Consuming excessive amounts of alcohol can increase your risk of systemic health issues that may contribute to an eye stroke, including high blood pressure and high cholesterol.
- Maintain a healthy lifestyle – Eating a healthy, balanced diet, getting regular exercise and maintaining a healthy weight can help lower your risk of systemic conditions associated with eye strokes.
Know when to get medical help
One of the most important factors involving strokes in the eye is seeking time-sensitive emergency care. Responding quickly to initial eye stroke symptoms, such as sudden painless vision loss or blurry vision, is key to reducing the risk or extent of permanent vision loss and improving visual outcomes.
If you or a loved one experiences any symptoms of an ocular stroke, go to your nearest hospital emergency room at once, even if the symptoms seem to improve.
Frequently asked questions about eye strokes
Suffering an eye stroke can be a frightening experience. But knowing what to expect can help ensure you’re prepared should you face this condition. Below are answers to questions people commonly have about ocular strokes:
Can an eye stroke lead to a brain stroke?
Yes. In fact, approximately 30% of eye stroke cases occur alongside a brain stroke. This also increases the risk of additional future strokes.
Can you die from an eye stroke?
An eye stroke, itself, is not usually life-threatening. However, it can be a sign of cardiovascular disease, which increases the risk of a heart attack and brain stroke.
Can your vision come back after an eye stroke?
An ocular stroke often causes at least some permanent vision loss. While vision may improve in certain cases, it may not recover to the level it was before the stroke.
Can you still drive after an eye stroke?
Whether you can still drive after having a stroke in your eye depends on how extensively your eyesight was affected. You must also meet your state’s legal vision requirements for driving. Your eye doctor can provide guidance and help determine if your vision is sufficient for you to drive safely.
READ NEXT: How a stroke can change your vision