Optic neuritis and neuropathy: Symptoms, causes, treatments
The optic nerve is the connection between the eye and the brain that transmits visual information from the retina. Inflammation of this nerve is called optic neuritis. During optic neuritis, inflammation can cause damage to the protective sheath (myelin) surrounding this nerve and the nerve itself. It can affect one optic nerve or both optic nerves at the same time.
Vision symptoms from optic neuritis can include blurring, blind spots or complete loss of vision. You also may notice distorted vision, reduced color vision and pain when you move one or both eyes. These types of symptoms may precede vision loss due to optic neuritis.
The term optic neuropathy more generally describes optic nerve abnormalities or damage. This damage could be from blocked blood flow, certain medical conditions or toxic exposure. Optic neuritis is one specific cause of an optic neuropathy.
What causes optic neuritis?
Optic neuritis can occur in anyone, but it usually occurs in adults younger than 45 and affects more women than men. The condition is common in people who have multiple sclerosis (MS), which occurs when the body's own immune system attacks and destroys protective nerve coverings.
Besides affecting eyesight, related nerve damage in MS can lead to loss of mobility and sensory functions, along with other debilitating conditions.
Other causes of optic neuritis include:
- Neuromyelitis optica spectrum disorder
- Anti-MOG Ab associatedsSyndrome
- Acute disseminated encephalomyelitis
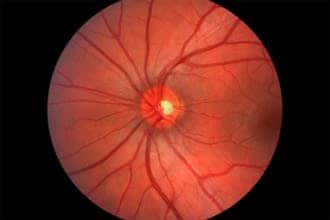
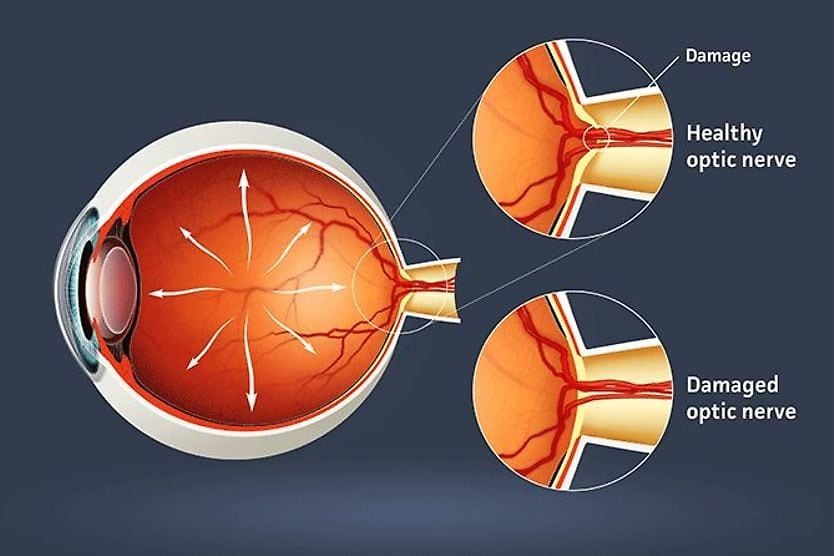
Image of the back of a healthy eye, where the optic nerve is located. When the optic nerve is damaged, poor vision result.
Other causes of optic neuropathy include:
- Infections (such as toxoplasmosis, cryptococcus, herpes simplex, Lyme disease)
- Other viral infections
- Neurological disorders
- Leber hereditary optic neuropathy, an inherited form of vision loss that mostly affects males in their 20s or 30s
- Certain medications (e.g., ethambutol, vigabatrin)
- Nutritional deficiency
- Toxins (including methanol, alcohol and tobacco)
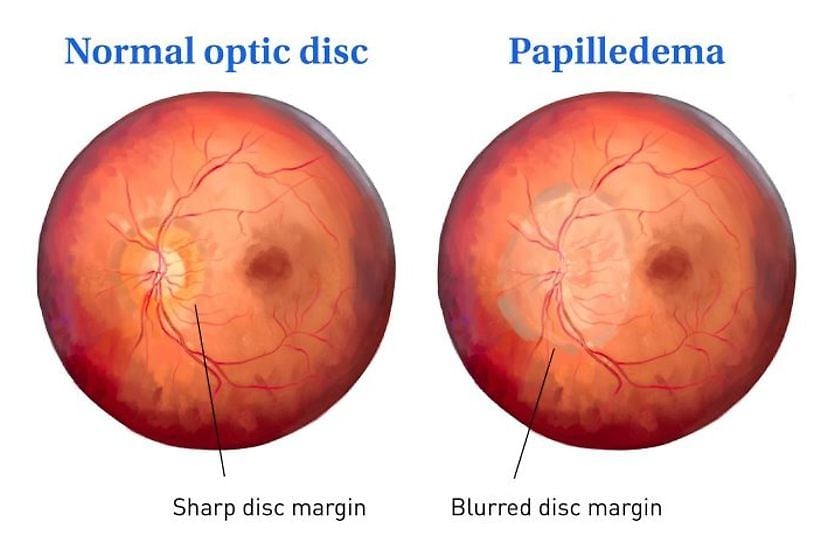
When optic neuritis is present, the pupil can react in an abnormal fashion (afferent pupillary defect). This means the pupil actually dilates instead of constricting in the presence of bright light. Depending on the severity of optic neuritis, the optic nerve may appear normal or swollen.
During an eye exam, your eye doctor may look for signs of optic neuritis by conducting tests to evaluate whether you have reduced vision, a red desaturation test (“red cap” test), visual field tests to determine if you have an enlarged blind spot (also known as a scotoma) and optical coherence tomography angiography (OCT/OCTA) to determine if there has been damage to the optic nerve fibers.
Your eye pressure will be measured, and your pupils may be dilated to provide a detailed view of the eye's interior structures, including the optic nerve and retina.
You may also be referred for an MRI of the optic nerves and the brain to detect possible underlying causes of optic nerve inflammation.
A person with optic neuritis usually undergoes an MRI of the brain to look for central nervous system lesions.
Treatments for optic neuritis
Treatment of optic neuritis has changed in recent years, due to a number of studies. These include Optic Neuritis Treatment Trials (ONTT).
In the ONTT, participants with optic neuritis were randomized for treatment with intravenous (IV) steroids, oral steroids or a placebo. Afterward, they were evaluated for several years.
From these studies, researchers learned that treatment with steroids had little effect on the final visual outcome as measured by high contrast visual acuity (black letters on a white background), but there was a benefit to vision when measured with more sensitive tests.
However, patients treated with high doses of steroids had fewer repeat attacks of optic neuritis than patients treated with low dose steroids alone. In fact, those treated with oral steroids alone had a higher risk of repeat attacks of optic neuritis than those treated with a placebo.
Even more importantly, patients treated initially with IV steroids had about half the risk of developing MS in two years as patients treated with oral steroids only or a placebo. Of those treated with IV (followed by oral) steroids, 7.5% developed MS in the following two years, versus about 16% in the other groups.
As a result of the ONTT, eye doctors now usually treat patients with a combination of IV and oral steroids or monitor the condition without prescribing medical treatment. Use of low dose steroids alone is not recommended.
For patients who are medically treated, the regimen typically includes three days of high dose steroids, followed by about 11 days of an oral steroid taper.
Additionally, patients with optic neuritis may be offered treatment with a procedure called therapeutic plasma exchange (TPE or PLEX). This therapy requires a patient to be connected to a machine for two to three hours. During this time, the patient’s blood is taken via an IV to the machine and certain plasma proteins are removed. The patient’s blood is then returned to them, having been “cleaned” of some of the immune system components that promote inflammation.
Prognosis for those who have optic neuritis
Visual changes from optic neuritis may worsen over the first week or so before stabilizing. Gradual improvement typically begins after that, and many people recover much of their vision within several months — though some recovery can continue over the course of a year.
Optic neuritis can recur, either in the same eye or in the other eye, which is one reason ongoing follow-up with an eye doctor matters. Identifying any underlying cause is also important, as recurrent episodes are sometimes preventable when a related condition is diagnosed and treated.
Because optic neuritis can sometimes be the first sign of multiple sclerosis (MS), your doctor may recommend an MRI to look for brain changes associated with MS. Long-term research from the ONTT found that, over a 15-year period, about 72% of patients with one or more lesions on their initial brain MRI went on to develop MS, compared with about 25% of patients whose MRI was normal.
Working closely with an eye doctor and a neurologist can help guide monitoring, treatment and long-term care.
READ NEXT: What is the optic disc