Leber congenital amaurosis: Risk factors, causes, symptoms and diagnosis

What is Leber congenital amaurosis?
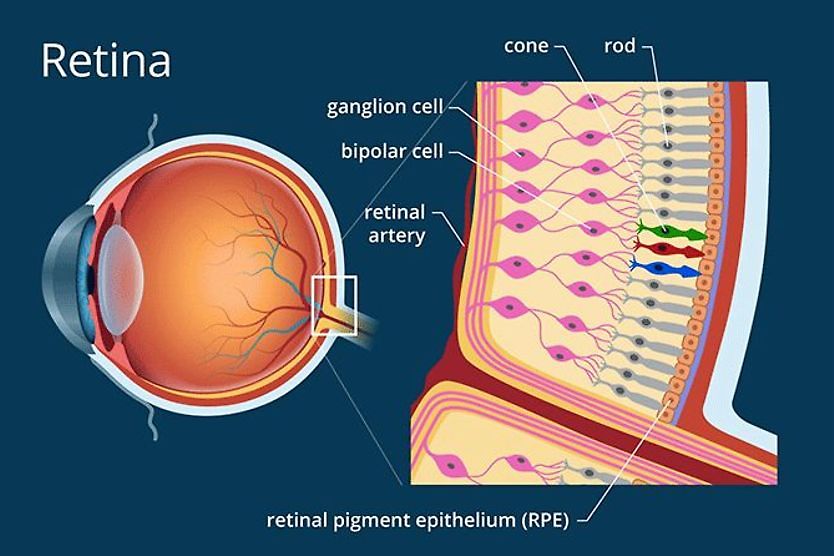
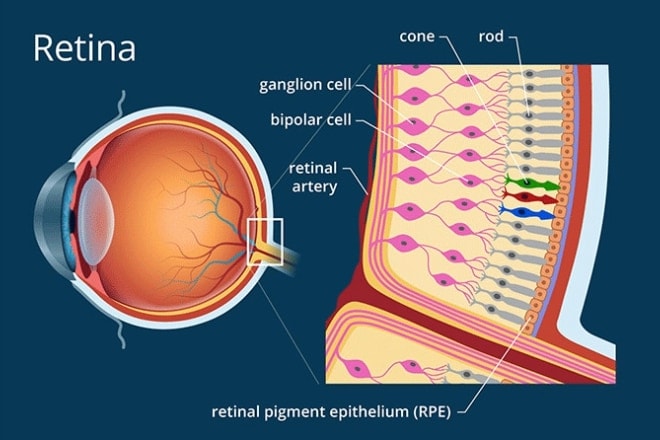
Leber congenital amaurosis (LCA) is a type of rare retinal dystrophy present at birth. It’s a genetic condition, meaning it’s passed down from parents to children. It affects specialized cells in the eyes that detect light, causing severe, gradual vision loss. The cells, called photoreceptors, are located in the retina. The retina is the light-sensing tissue at the back of the eye.
LCA is caused by changes in specific genes. These genes provide instructions for making proteins needed for retinal development. When these genes are mutated, the proteins are defective or missing. This prevents the retina from properly:
- Detecting and processing incoming light.
- Converting light into interpretable signals for the brain.
- Maintaining the health and function of photoreceptor cells.
How common is LCA?
It is estimated that LCA may affect 1 to 2 in every 100,000 people worldwide. It makes up only 5% of all retinal dystrophies. However, it may lead to 1 in 5 cases of childhood blindness in school-aged kids.
Are there different forms of LCA?
There are different forms of Leber’s congenital amaurosis depending on which gene is affected. Children with LCA can have very different levels of vision early on. This can range from having some useful sight to blindness. Some children with particular gene changes may have better vision initially. These children may be diagnosed with "early-onset retinal dystrophy" instead of LCA. However, eyesight typically worsens over time in all children with LCA.
Are there treatment options for LCA?
Early diagnosis and gene therapy treatment may help preserve vision in some children with LCA. The treatment is determined by the form of LCA.
For example, one form caused by two abnormal RPE65 genes may be treated with voretigene neparvovec-rzyl. This is an FDA-approved gene therapy for this inherited eye disease. Additional types of treatments and clinical trials may also be available. These are discussed further in the treatment section.
Signs and symptoms
Poor vision typically becomes noticeable within the first six months of life. Some children may often rub or poke their eyes to stimulate light sensations in the retina. This is called Franceschetti's oculo-digital sign. It may lead to the eyes slightly sinking into the eye socket.
What are the early signs?
Caregivers may observe that their baby doesn't respond visually. Often, children showing early signs of LCA may exhibit the following:
- Do not appear to focus on objects.
- Do not track moving objects with their eyes.
- Have involuntary, jerky eye movements (infantile nystagmus).
- Have a sluggish pupil response.
- Experience light sensitivity (photophobia).
Additional signs and symptoms
Children with LCA also may develop:
- Severe farsightedness
- Night blindness
- Vision loss
- Cone-shaped corneas (keratoconus)
- Cataracts
- Deterioration of cells in the central retina (macular atrophy)
- Crossed eyes (strabismus)
- Abnormal eye pigmentation
- Issues with their ability to smell
- Slower developmental progress (very rare)
Genetics and LCA development
Leber congenital amaurosis is caused by mutations in specific genes. These genes tell the body how to make proteins that are key to normal retinal development.
How is the retina affected?
In LCA, the mutated genes produce proteins that are faulty or absent. As a result, retinal cells are missing essential proteins. This can affect the retina's ability to:
- Detect and process light.
- Convert light into signals that the brain can interpret.
- Maintain the health and function of photoreceptor cells.
- Process vitamin A, which is crucial for normal vision.
The retina can look different in each child. Some may appear nearly normal, while others may show clear signs of damage.
What genes are involved in LCA?
Scientists have found approximately 30 different genes associated with LCA. There are still genes that have not yet been identified that are responsible for LCA. The genes most frequently involved in LCA may include:
- CEP290 (15% of cases)
- GUCY2D (12% of cases)
- CRB1 (10% of cases)
- RPE65 (8% of cases)
The inheritance pattern of LCA
LCA typically follows an autosomal recessive inheritance pattern. This means that for a child to develop the condition, they must inherit two copies of the mutated gene — one from each parent. Both parents typically have normal vision because they carry only one copy of the mutated gene alongside one normal working copy.
In LCA, when children inherit two copies of the mutated gene, their cells cannot produce the necessary proteins correctly. Without these key proteins, the photoreceptor cells in the retina start to fail and slowly break down.
Researchers are creating therapies to try to restore protein function. These therapies may help preserve or improve vision in children with specific types of LCA.
Diagnosis
Diagnosing LCA may require a thorough eye examination and specialized testing performed by an eye doctor. Eye doctors may run tests to make sure symptoms are not caused by other similar conditions, such as retinitis pigmentosa.
Eye exam
The eye doctor may perform a detailed eye exam, looking for signs such as:
- Nystagmus
- Light sensitivity
- Retinal changes
Early on, the retina might look normal. Changes may become more obvious as the condition progresses. LCA cannot typically be diagnosed with just an eye exam, and specialized tests are typically required.
Electroretinogram
An electroretinogram (ERG) is a typically painless test to see how the retina responds to light.
- It measures the retina’s electrical activity.
- Results are “flat” in LCA (meaning the retina is not working properly).
Genetic testing
Genetic testing can confirm LCA and identify the specific gene in over 75% of cases. Testing:
- Allows doctors to recommend treatments or clinical trials.
- Helps families understand how LCA is passed down and what the chances are that future children may also have LCA.
Optical coherence tomography
Optical coherence tomography angiography (OCT / OCTA) uses light waves to take detailed images of the different layers of the retina.
- It can show early changes as well as degeneration of the retina over time.
- Specific OCT patterns are linked to specific gene mutations.
How is Leber congenital amaurosis different from Leber hereditary optic neuropathy?
Leber hereditary optic neuropathy (LHON) and Leber congenital amaurosis both can impact vision. However, they are different genetic eye conditions. LHON typically affects vision and causes vision problems after early childhood, most often in the teens or 20s.
Treatment options
New therapies are becoming available for LCA. Ongoing research means more people may be able to access treatments.
Getting the right diagnosis
Before any treatment, doctors need to know exactly which gene is involved. This is critical because:
- It helps match each patient to the right therapy.
- Genetic counselors can explain inheritance and guide family planning.
Approved gene therapy
A major breakthrough in treating LCA is gene therapy. It aims to correct the mutated gene by delivering healthy copies into retinal cells.
Voretigene neparvovec-rzyl for RPE65-LCA **
Voretigene neparvovec-rzyl is an FDA-approved gene therapy for this inherited eye disease. It is for patients one year and older who have mutations in both copies of the RPE65 gene. This form of LCA typically develops later in life. It can initially impair low-light vision, making it difficult to see in poorly lit environments. Over time, vision may deteriorate under all light levels.
Important facts about voretigene neparvovec-rzyl:
- It can only work when there is still some functioning retina.
- A virus is used to transport a healthy copy of the RPE65 gene into the retinal cells.
- The treatment is delivered during a surgical procedure called a vitrectomy, which is performed in an operating room.
- Patients may see improvement in low-light conditions, though the treatment typically does not restore completely normal vision.
- The effects of the treatment have been shown to last for several years in some patients after the procedure.
Gene therapy clinical trials
Several gene therapy candidates for LCA are in the research and development phase.
Examples of clinical trials include:
EDIT-101 for CEP290-related LCA
Researchers are testing a new gene editing candidate that works by correcting a specific problem in the CEP290 gene. In early studies, around two-thirds of participants were reported to have improved their vision or mobility. This trial has been paused.
QR-110 for CEP290-related LCA
Scientists are exploring a different approach for CEP290-related LCA. This proposed treatment is called QR-110. This therapy uses specially designed molecules to help the gene work better.
Gene therapy for AIPL1-related LCA
Researchers in the UK tested a gene therapy candidate in children with AIPL1-related vision loss. The treated eye was reported to have shown improvements in vision and brain responses to visual signals. However, the untreated eye reportedly continued to decline.
GUCY2D gene therapy
Another study is testing a treatment for people with mutations in the GUCY2D gene. After one year, some participants were reported to have showed better mobility in low-light conditions. They also were reported to have improved their ability to detect light.
LCA5 gene therapy
Scientists are investigating a gene therapy candidate for LCA5-related vision loss. This therapy targets a protein called lebercilin. It helps transport important materials within the light-sensing cells of the eye.
RDH12 gene therapy
Additional gene therapy studies for RDH12-related LCA are planned.
New clinical trials may mark important steps in developing treatments for LCA. Research on other types of therapies is also underway.
Living with Leber congenital amaurosis
Living with Leber’s congenital amaurosis may present challenges that can affect all aspects of life. Doctors at teaching or university hospitals can help with diagnosis and care. This includes eye doctors, geneticists, counselors and pediatricians. Families can also benefit from nonprofit support networks and resources.
Children diagnosed with LCA often begin learning adaptive techniques early in life. Many aids, support services and training programs may help boost independence and progress. These may include:
Early support
- Mobility training (white cane, guide dogs)
- Braille and tactile reading lessons
- Occupational therapy for daily tasks at home and school
Lighting and contrast
- Brighter lighting in the home and portable lighting, such as flashlights
- Glare reduction to decrease strain
- Higher contrast, such as black items on a white surface or dark, bold markers
Low-vision aids
- Strong glasses, hand-held magnifiers and reading prisms
- Telescopic glasses for distance vision
Assistive technology
- Screen-readers and text-to-speech apps on computers and phones
- Optical character recognition apps that convert printed words into speech
- GPS-based guides that give audio directions outdoors
Children with LCA may have severe vision problems from birth or early childhood. This is because their retinal cells are missing essential proteins for normal vision. Supportive programs and dedicated health care teams can offer help for those affected. With new advances, families can maintain hope for innovative therapies that may enhance vision in the future.
If you suspect your child has problems with their vision, it is recommended to schedule a comprehensive eye exam for them with an eye doctor near you.