Glaucoma and what it means to be a glaucoma suspect


Are you a glaucoma suspect?
A glaucoma suspect exhibits risk factors. Factors include higher pressure in the eye, age or history that put them at higher risk of developing optic nerve damage or vision loss. Glaucoma can cause vision loss without early symptoms, so doctors will note someone is a glaucoma suspect to monitor them for it.
What does it mean to be a glaucoma suspect?
Your eye doctor is looking at the following clinical signs when monitoring for the development of primary open-angle glaucoma (POAG). POAG is the kind that most Americans have.
If your doctor told you that you are a glaucoma suspect, it means that they found one or more of the following during your eye exam:
- High intraocular pressure (IOP)
- Abnormal optic nerve appearance
- Retinal nerve fiber layer abnormalities
- Visual field defect
- Abnormal drainage angle
What risk factors increase the risk of developing glaucoma?
These risk factors can increase the risk of developing glaucoma:
- Age – People over age 60 are at increased risk for the disease.
- Family history – Having a close relative with glaucoma increases the risk of developing glaucoma.
- Race – African Americans are at an overall higher risk of glaucoma. In addition, they are at a higher risk of experiencing permanent vision impairment. African Americans are also at increased risk after age 40 rather than 60. Asian Americans and Native Alaskans have a higher risk of a type of glaucoma called angle closure. Japanese Americans are at higher risk of developing low-tension glaucoma.
- Certain diseases – Diabetes, heart disease and high blood pressure have been found to increase the risk of developing glaucoma.
- Eye trauma – An injury to the eye can result in a sudden increase in eye pressure. It can also increase the chance of having high eye pressure later. The drainage angle could also close if the injury displaces the lens, resulting in increased pressure.
- Certain eye conditions – Thin corneas, a tumor in the eye, a retinal detachment, episodes of eye inflammation or high myopia may increase the risk of glaucoma.
- Long-term corticosteroid use. Extended use of cortisone, hydrocortisone and prednisone can increase the risk of secondary glaucoma.
Do glaucoma suspects always develop glaucoma?
No, not all glaucoma suspects will develop glaucoma. Your eye doctor will note that you are a glaucoma suspect in your chart so that they can monitor you for developing it.
A note will be made after an exam and review of your family history if they indicate you may be at higher risk for developing it in the future. Glaucoma can cause gradual vision loss in the periphery of your vision that can be so subtle that an individual may not notice it.
About three million Americans have been diagnosed with glaucoma. Vision loss from glaucoma is permanent, and it is one of the leading causes of blindness for adults over 60. By noting that you are a glaucoma suspect, your doctor will begin to follow you more closely. They will look for signs of glaucoma so they can catch the disease early and prevent vision loss.
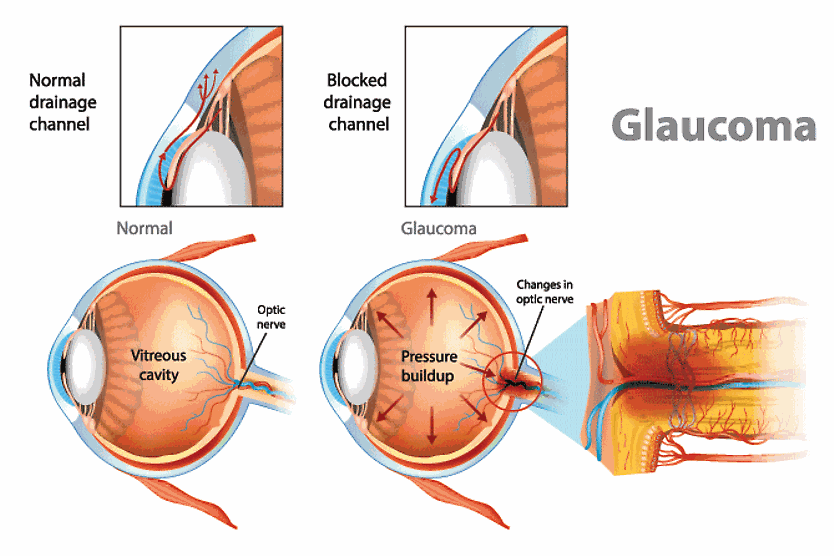
What is glaucoma?
Glaucoma is a set of eye conditions that damage the optic nerve, which connects the eye to the brain. Typically, this damage is due to pressure in the eye that is too high. Although, there is a type of glaucoma that can cause optic nerve damage even with normal eye pressure.
Your doctor can tell you what type of glaucoma you are being monitored for. The different types of glaucoma include:
Primary open-angle glaucoma (POAG) – This is the most common form of glaucoma. In this type of glaucoma, the fluid that fills the front of the eye (the aqueous humor) has increased resistance as it flows out of the drainage system. Backup of fluid results in chronically increased pressure within the eye.
Normal tension glaucoma (NTG) – This is considered a type of open-angle glaucoma by most eye doctors, but the IOP is in the normal range. It is classified as glaucoma because of clinical signs of optic nerve damage, retinal nerve fiber layer thinning or loss of peripheral vision that is typical of glaucoma.
Closed-angle glaucoma (CAG) – This less common form of glaucoma is also known as narrow-angle glaucoma or angle-closure glaucoma. It is due to a narrowing or blockage of the angle (where the aqueous drains) between the cornea and iris. As a result, the aqueous cannot properly drain out of the eye.
- Acute angle-closure glaucoma – This type of glaucoma is due to sudden blockage of the drainage angle. Someone experiencing an acute attack may feel severe pain, headache, blurry vision with halos, and nausea or vomiting. This is an eye emergency.
- Chronic angle-closure glaucoma – This type of glaucoma can also occur over time, slowly damaging the optic nerve. It may be due to a large lens, thick iris, or other reasons that narrow the drainage angle. One-third of people with this type of glaucoma will experience an acute angle-closure attack.
Secondary glaucomas – Secondary glaucomas develop secondary to another eye or medical condition. The types of glaucoma in this category include:
- Neovascular glaucoma – This type of glaucoma is usually a complication of central retinal vein occlusion or diabetic retinopathy, resulting in certain factors that cause abnormal, leaky blood vessels to grow in the retina. These factors travel to the iris and drainage angle and cause abnormal blood vessels to grow there as well. This leads to decreased drainage of the aqueous humor and increased IOP.
- Glaucoma caused by trauma – A direct injury to the eye can result in acute angle closure glaucoma or a delayed (chronic) onset of glaucoma, which develops over time due to complications from the injury.
- Glaucoma due to surgery – Complications from surgery can result in elevated IOP both suddenly (acute) and over time (chronic).
- Pigment Dispersion Syndrome – This type of glaucoma develops 3x more often in men than women. It is the result of pigment that breaks off the back of the iris (the colored part of the eye) and obstructs the drainage canals.
- Pseudoexfoliation syndrome – This type of glaucoma occurs when white flecks of protein flake off the eye's lens and accumulate in the eye’s drainage system, clogging it.
What is a glaucoma follow-up visit like, and how often will it be?
If you are a low-risk glaucoma suspect, your doctor will likely want to see you every six to 12 months. If your risk is higher, your doctor will likely want to see you more frequently.
At your glaucoma monitoring follow-up visit, your doctor will examine:
- Eye pressure
- Vision
- Retina and optic nerve
- Images of your optic nerve and retinal nerve fiber layer
- Visual field testing results
If at some point your doctor determines that you need treatment for glaucoma, initial treatment is typically with eye drops or laser surgery to increase the drainage of the aqueous out of the eye. These treatments lower the pressure in the eye and decrease the risk of vision loss.
Glaucoma is a complex condition, and treatment for it is equally complex. A glaucoma specialist will consider many factors when beginning treatment and determining the course of treatment.
What can I do to decrease my risk of glaucoma?
Some risk factors for glaucoma, such as your family history, age, and how your eye is built, cannot be changed. There are other things that you can do to reduce your risk of vision loss and maintain your eye health:
- Get routine comprehensive eye exams, and go to your follow-up appointments.
- Eat a diet rich in nutritious whole foods, including green leafy vegetables and colored fruits and vegetables.
- Establish a safe and effective exercise routine. But, excessive exercise, lifting weights or head down positions can raise eye pressure, so speak to your eye doctor about any exercise you should avoid.
- If you have been prescribed steroid medication, let your doctor know if you are a glaucoma suspect.
- Wear protective eyewear.
If your eye doctor has told you that you are a glaucoma suspect, the best way to decrease your risk of vision loss from glaucoma is by following their recommendations on routine follow-up care.