Can you be short-sighted in one eye and long-sighted in the other?
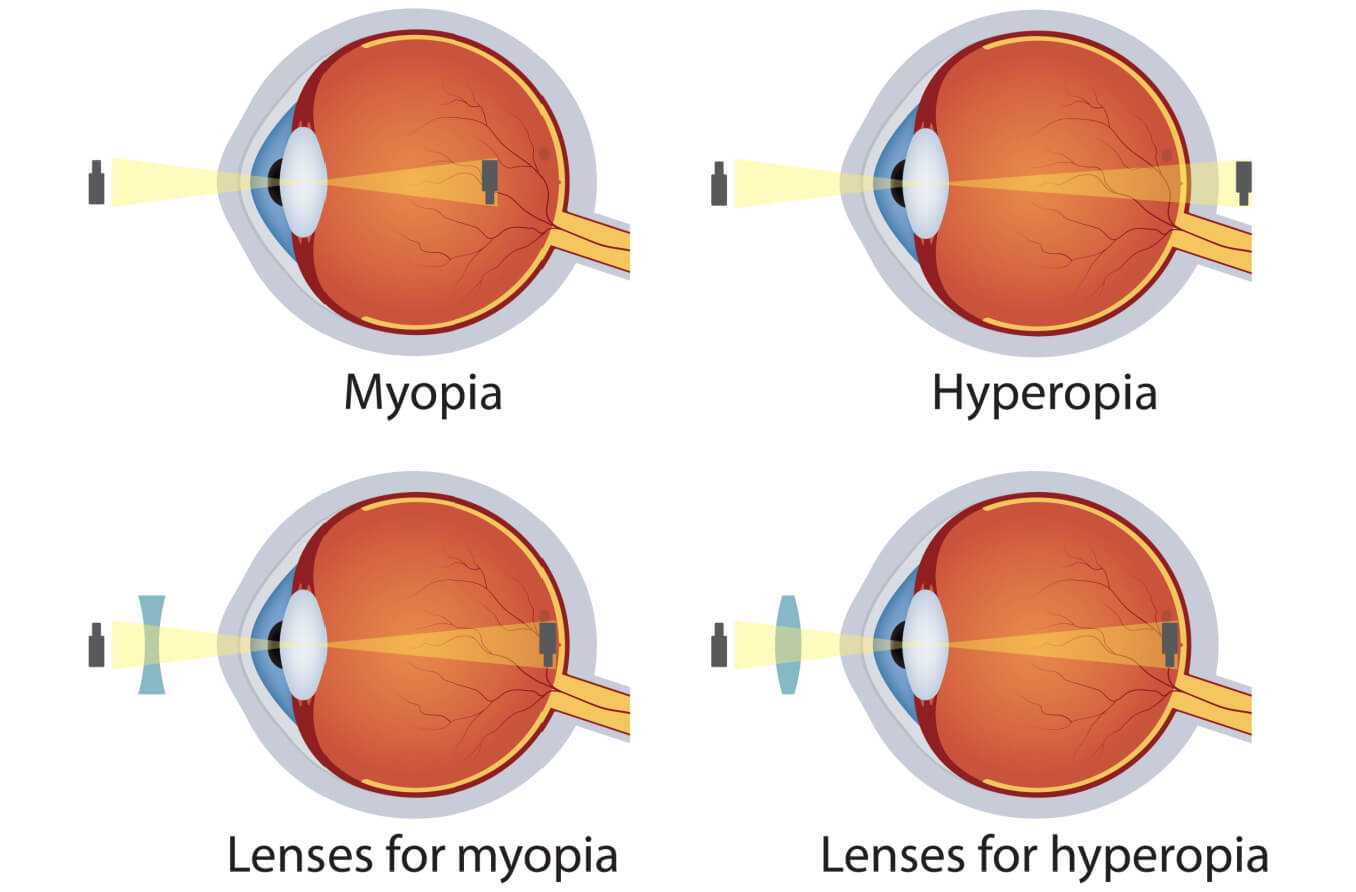
Yes, people can be short-sighted in one eye and long-sighted in the other. The medical terms for this condition are anisometropia and antimetropia. Anisometropia means the two eyes have a difference in refractive power. Antimetropia means the difference is myopia in one eye and hyperopia in the other.
In anisometropia, both eyes may be short-sighted or long-sighted or, one eye can be short-sighted and the other long-sighted.
If you have anisometropia, your prescription for one eye will differ from the other eye by one dioptre or more.
Antimetropia is the term used specifically for myopia in one eye and hyperopia in the other. However, some optometrists may use the term mixed anisometropia for this condition.
Anisometropia symptoms
Anisometropia usually impacts the ability of the two eyes to work together. People with uncorrected anisometropia often have reduced vision for tasks like reading. They will also notice unequal blur in the two eyes at different distances. Other symptoms of anisometropia include:
Frowning
Excessive amounts of blinking or eye rubbing
Poor depth perception
Problems with the focusing ability of their eyes (accommodation)
Nausea
Adults with uncorrected anisometropia might notice they struggle at work. Jobs that require excellent vision and depth perception can pose difficulties for people with anisometropia.
In some cases, anisometropia can be present without any symptoms. This makes it very important for children to have regular eye exams. Even without symptoms, anisometropia can cause other complications.
In children, the brain will often learn very quickly to favour the eye with the lower refractive error. This is the brain's way of reducing these symptoms, but it can lead to amblyopia (“lazy eye”) in the other eye.
Children may also close, block or even cover one eye to "fix" the difference in vision between the two.
Correcting anisometropia
It is critical to diagnose and correct anisometropia as early as possible. If the brain is allowed to "ignore" the one eye for too long, it can cause irreversible amblyopia.
Regular eye exams in pre-school and primary school are essential. They allow the optometrist to rule out anisometropia and ensure typical visual development.
Anisometropia can be corrected with glasses, contact lenses and even refractive surgery.
When unequal refractive errors are corrected with glasses, objects seen by one eye look larger or smaller than they do with the other eye. This difference in image sizes is called aniseikonia. This, too, can cause problems with eye strain, headaches, difficulty reading and double vision.
Glasses often aren't a good solution when the degree of anisometropia is high. In this case, contact lenses are usually the treatment of choice. This is true even for young children.
Contact lenses cause little or no aniseikonia because they rest on the surface of the eye. They can provide more comfortable and natural-looking vision than glasses.
LASIK is another option to correct anisometropia but this should only be considered after the refractive errors are stable, generally after age 24.
The first step in detecting whether your child has anisometropia is an eye test. Schedule a comprehensive eye exam with an optometrist near you.
Borish's clinical refraction. Benjamin WJ & Borish IM. St. Louis Mo: Butterworth Heinemann/Elsevier. 2006.
Emmetropization, refraction and refractive errors: Control of postnatal eye growth, current and developing treatments. In Hoyt CS & Taylor D (eds) Pediatric Ophthalmology and Strabismus. Fourth Edition. WB Saunders. 2013.
Aniseikonia and anisometropia: Implications for suppression and amblyopia. Clinical and Experimental Optometry. January 2019.
The correlation between headache and refractive errors. Journal of American Association for Pediatric Ophthalmology and Strabismus. March 2008.
Ametropia in children with headache. Pakistan Journal of Medical Sciences. May - June 2019.
Page published on Tuesday, 17 March 2020
Page updated on Friday, 4 August 2023
Medically reviewed on Thursday, 20 January 2022