Vision surgery for presbyopia
Sometime after age 40, we all start having trouble reading small print. This (perfectly normal) "aging eye" change is called presbyopia.
In the past, the only solutions for presbyopia were reading glasses or bifocals. But thankfully, there now are many ways to overcome the challenges of presbyopia — including a variety of surgical options that can help you maintain a glasses-free lifestyle.
Here's a summary of presbyopia surgery options currently available:
1. Corneal Inlays
Corneal inlays are an exciting new option for the correction of presbyopia. These tiny lenses are implanted in the cornea of one eye to improve near vision without causing any significant loss in distance vision.
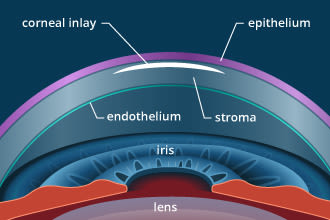
Corneal inlays for presbyopia correction generally are placed in the anterior portion of the corneal stroma of the non-dominant eye.
A corneal inlay procedure generally takes only about 10 to 15 minutes. A small pocket is created in the cornea with a femtosecond laser, and the surgeon positions the inlay over the center of the pupil. The corneal pocket seals on its own without stitches.
In addition to being minimally invasive, corneal inlays can be removed and replaced if visual results aren't as clear as desired.
The only FDA-approved corneal inlay currently available for use in presbyopia surgery performed in the U.S. is the Kamra inlay, marketed by AcuFocus. [Read more about corneal inlays.]
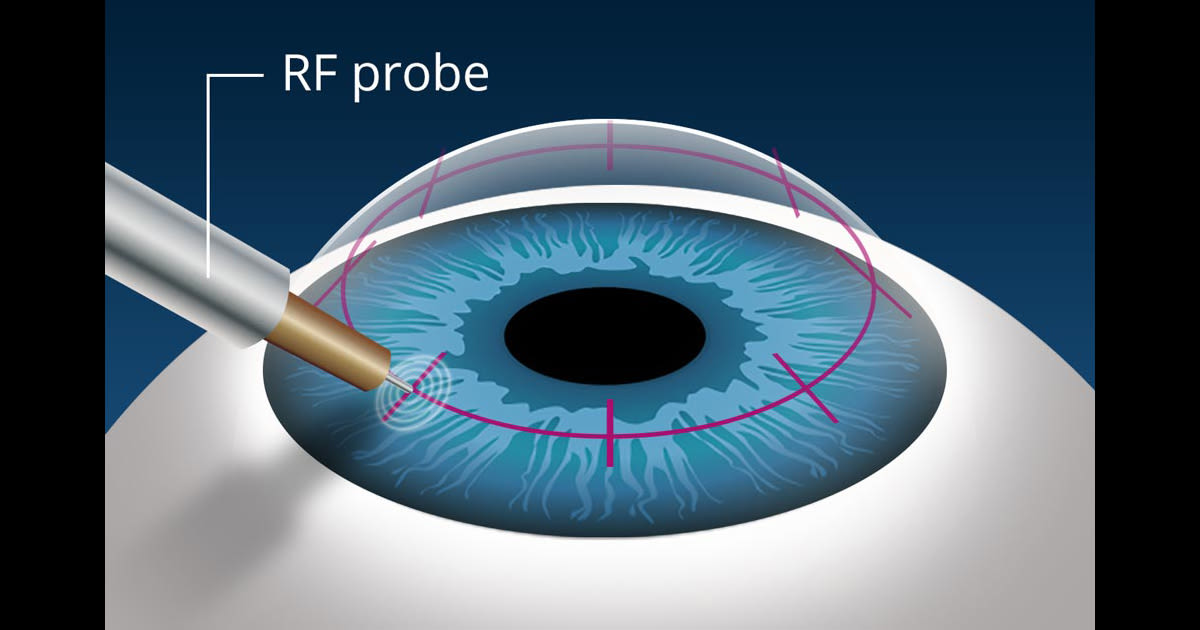
2. NearVision CK
NearVision CK is a minimally invasive surgical procedure that uses radio-frequency (RF) energy to change the shape of the cornea and provide sharper near vision without glasses.


Developed by Refractec, NearVision CK was the first surgical procedure to gain FDA approval for the correction of presbyopia, which occurred in March 2004.
NearVision CK is a monovision technique — meaning one eye is made nearsighted by the procedure (for improved close-up vision) while the other eye remains untouched.
The limitation of monovision is that the eye that sees clearly up close will be blurry in the distance. But with both eyes open, most people can adapt to this and feel their vision is acceptably clear at all distances.
Still, it's a good idea to first try monovision with contact lenses or a trial lens in the doctor's office before proceeding with NearVision CK, to make sure you'll adapt.
Another limitation of NearVision CK is that the vision improvement from the procedure tends to diminish after several months and the procedure may need to be repeated. [Read more about NearVision CK.]
3. Monovision LASIK
If you've successfully tried monovision with contact lenses and want a more permanent monovision correction than NearVision CK, you may be a good candidate for monovision LASIK.
Monovision LASIK generally is recommended for presbyopia only if you also have refractive errors (nearsightedness, farsightedness and/or astigmatism) that will be treated with the procedure.
People who choose monovision LASIK generally are pleased with their distance and near vision without glasses most of the day. But often, a pair of reading glasses is still recommended for very small print; and many who undergo the procedure find a pair of glasses for driving at night also is helpful.
4. Refractive Lens Exchange
Refractive lens exchange (RLE) is a more invasive procedure that can be used for presbyopia correction. In this procedure, the eye's natural lens is removed and replaced with an intraocular lens (IOL) that's identical to the type of IOL used in cataract surgery.

(The only difference between RLE and cataract surgery is that refractive lens exchange is performed before the natural lens of the eye becomes clouded with a cataract. Although refractive lens exchange is not FDA-approved specifically for presbyopia correction, it may be available "off label" for qualified candidates. Ask your eye surgeon for details.)
RLE can correct presbyopia by replacing the eye's natural lens with a multifocal IOL or an accommodative IOL. In addition to providing clear distance vision, these premium intraocular lenses help restore near vision as well. [Read more about refractive lens exchange.]
Consult With Your Eye Doctor First
The first step in finding the best solution to presbyopia for your needs — including surgery for presbyopia — is to have a consultation with your eye doctor following a comprehensive eye exam.
Your doctor can help you choose what makes the most sense for you based on important factors including your age, eye health and your daily visual needs.
Page published on Wednesday, February 27, 2019