Intraocular lens implants (IOLs): Lens replacement surgery
What is an IOL implant?
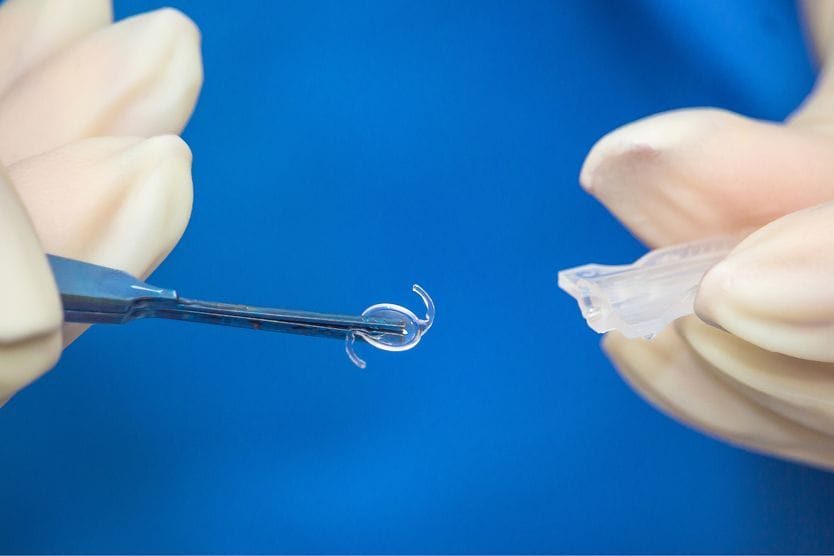
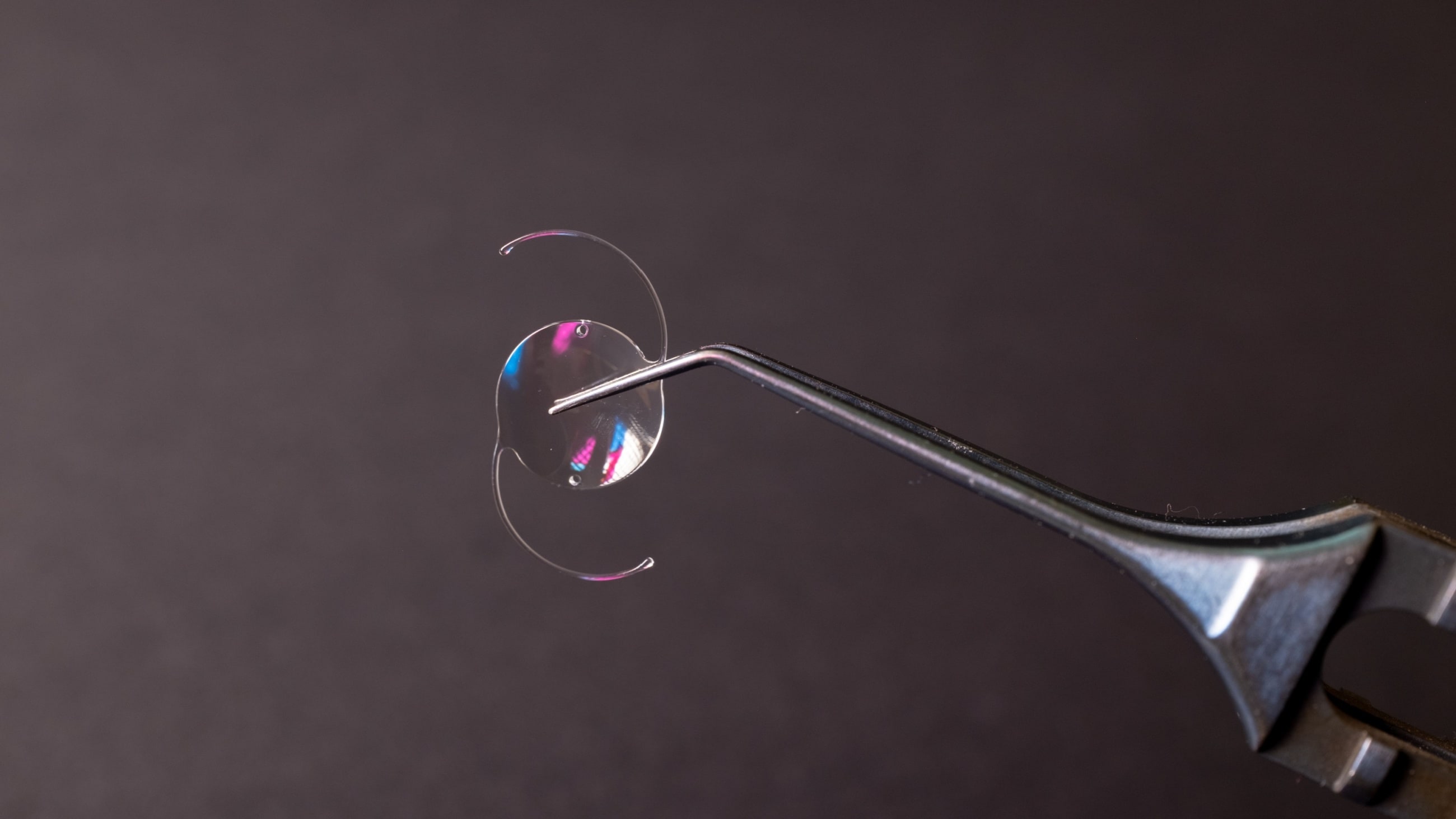
An intraocular lens (IOL) is a clear, artificial lens an eye doctor implants inside your eye. Most IOLs are used to replace your eye's natural lens if you have cataracts. Doctors may also use IOLs to correct your vision even if you don't have cataracts. This is called refractive lens exchange.

The tiny, clear IOL replaces the natural lens inside your eye.
Refractive lens exchange (RLE) and cataract surgery are very similar.
There's a good chance you know at least one person who already has an IOL implant. Lens replacement surgery for cataracts is a common procedure worldwide.
How IOLs work
Your clear natural lens focuses light inside your eye. Everything would look blurry if you didn't have a lens.
When someone has a cataract, the lens is cloudy, and it scatters light inside the eye. If they become advanced or “mature” it can block light completely. These problems can cause blurry vision, washed-out colors, vision impairment, glare and halos around lights or other symptoms.
Refractive errors usually happen because your eye is too short or too long. They're also caused by lens aging and the shape of the front layer of your eye.
They make your vision blurry, too.
The common refractive errors are:
An IOL implant may fix the symptoms caused by your original lens. It can compensate for refractive error, too.
The IOL corrects your vision by helping light focus inside your eye. The lens implant will be set to your custom measurements to help you see as clearly as possible.
What is an IOL made of?
Most IOLs are made of special kinds of plastic. The materials include:
- Acrylic (most common)
- Collamer
- Silicone
Types of IOLs
There's more than one type of intraocular lens. Each one can help a different aspect of your eyesight.
Monofocal IOLs
Monofocal lenses are a popular IOL. They correct your vision for one distance: near, medium or distant.
The majority of people have their IOLs set to help their distant vision. In that case, you would still need to wear prescription glasses or readers if you already needed them beforehand.
Multifocal IOLs
A multifocal IOL has different focus zones on the lens. This helps you focus at more than one distance.
They're often used for people with presbyopia (difficulty reading without glasses).
It can take a while to get used to multifocal lenses. Some people say they see more halos around bright lights with this lens implant, but they typically go away in most people.
Accommodating IOLs
An accommodating IOL can also help you focus on both near and far distances. But it doesn't work the same way a multifocal IOL does.
Instead of using special focus zones on the lens, accommodating lenses move or change their shape to help you see better.
Toric IOLs
Toric IOLs are monofocal or multifocal lenses that help people with astigmatism. The surgery is a little different because the doctor needs to make a special marking to rotate and align the IOL implant inside your eye to ensure clear vision.
Monovision
Sometimes it can help to have two monofocal lenses set to a different distance in each eye. This is called monovision.
Monovision IOLs help some people see near and far objects more clearly. It isn't easy in some cases to adapt to them, so an eye doctor could ask you to try monovision contact lenses first.
Phakic IOLs
Unlike most other intraocular lenses, a phakic IOL isn't used as an eye lens replacement. They usually aren't used for people with cataracts, either.
Phakic lenses are one alternative to surgeries like LASIK. The implant is placed in front of or just behind your natural lens to correct nearsightedness, so you still retain your natural lens.
How lens replacement surgery works
The doctor will generally follow these steps during lens replacement surgery:
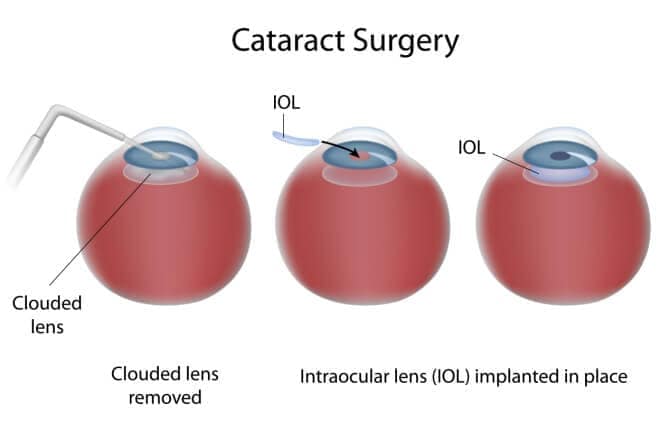
- Use eye drops to numb your eyes.
- Make tiny openings in the clear, front layer of your eye.
- Use a device to break up your natural lens into small pieces.
- Use suction to gently remove the lens pieces.
- Place the new IOL where your natural lens used to be.
- Place a shield over your eye to help protect it while it heals.
You'll be awake for the majority of the procedure with what is called conscious sedation or “twilight” anesthesia, but there is typically little to no pain. Depending on your health and mental status, you might require general anesthesia which will make you unconscious with breathing assistance. Your eye doctor will inform you of the type of anesthesia medically necessary for your procedure.
The small wound should heal on its own without any stitches. As your eye heals, the replacement lens should make your eyesight better than it was before surgery.
READ MORE: What you can expect before, during and after cataract surgery
IOL FAQs
What's the lifespan of an IOL?
IOLs are permanent, so they don't need to be replaced after a certain amount of time. They're designed to last for the rest of your life.
Is an IOL the only way to treat a cataract?
Yes. Right now, an intraocular lens implant is the appropriate way to fix the vision problems caused by a cataract.
Is lens replacement surgery safe?
Yes, it's very safe.
As with any surgery, complications can happen. You could be at higher risk if you have other eye or health problems. Talk to your eye doctor about any concerns before your procedure.
A "secondary cataract" is the most common side effect, but it's usually easy to treat.
What's the success rate for IOL surgery?
The success rate is about 97%. In other words, around 97 in every 100 patients will see more clearly once they recover from their procedure.
What's the recovery time for lens replacement surgery?
Some people notice their vision recovers within a few days of their procedure. For others, it could take a few weeks.
Your eye may feel gritty or watery while you heal. It might look bloodshot too.
Are IOLs covered by insurance?
Insurance may cover standard monofocal IOLs (and surgery) for cataracts as long as you meet their requirements. The claim will be processed by your health insurance, not vision insurance.
Premium lenses and refractive lens exchange surgery are less likely to be covered.
How much does an IOL cost?
The total cost of your IOL(s) and surgery will depend on several things. This could include the type of procedure, type of IOL, insurance coverage and other factors.
Your doctor's office will give you an estimate for any out-of-pocket costs before you have surgery.
READ NEXT: Does Medicare cover cataract surgery?